
World Diabetes Day 2023
Executive summary
* Each year, November 14th is World Diabetes Day.
* This World Diabetes Day we look back at progress over the past 10 years.
* The International Diabetes Federation (IDF) definition of diabetes has barely changed. The definition mentions the word “glucose” five times and acknowledges that all carbohydrate foods are broken down into glucose.
* The latest definition of diabetes has added gestational diabetes as a third type alongside Type 1 diabetes (T1D) and Type 2 diabetes (T2D).
* The IDF estimated that 371 million people had diabetes in 2013. Ten years later, they estimate 537 million people have diabetes. Forecasts for the next 10 years predict this rising to over 700 million. This is not a condition being improved globally.
* Progress has been made in research over the past 10 years. Trial evidence now exists to show that very low calorie or very low carbohydrate diets can put T2D into remission.
* The IDF and American Diabetes Association advice does not reflect this evidence. Dietary advice to avoid fat and consume carbohydrates prevails.
* This diet advice emanates from the long held fear of fat. This fear is without evidence base, but it is obstructing progress – particularly in the field of diabetes, although for other health conditions too.
Introduction
Each year, the 14th of November is World Diabetes Day. I have done something to mark this day on six previous Monday notes (Ref 1). The first was in 2013 (Ref 2). Let’s see if any progress has been made in the past 10 years.
The definition of diabetes
In the 2013 note, I opened with the definition of diabetes according to The International Diabetes Federation (IDF):
“Diabetes mellitus, or simply diabetes, is a chronic disease that occurs when the pancreas is no longer able to make insulin, or when the body cannot make good use of the insulin it produces.
Insulin is a hormone made by the pancreas, that acts like a key to let glucose from the food we eat pass from the blood stream into the cells in the body to produce energy. All carbohydrate foods are broken down into glucose in the blood. Insulin helps glucose get into the cells.
Not being able to produce insulin or use it effectively leads to raised glucose levels in the blood (known as hyperglycaemia). Over the long-term high glucose levels are associated with damage to the body and failure of various organs and tissues.”
The 2023 definition has shortened a couple of sentences, but it has not changed otherwise (Ref 3):
“Diabetes is a chronic condition that occurs when the pancreas can no longer make insulin, or the body cannot effectively use insulin.
Insulin is a hormone made by the pancreas that acts like a key to let glucose from the food we eat pass from the bloodstream into the cells in the body to produce energy. The body breaks down all carbohydrate foods into glucose in the blood, and insulin helps glucose move into the cells.
When the body cannot produce or use insulin effectively, this leads to high blood glucose levels, called hyperglycaemia. Over the long-term high glucose levels are associated with damage to the body and failure of various organs and tissues.”
Note the mention of the word “glucose” five times and the acknowledgment that all carbohydrate foods are broken down into glucose.
The different types
In 2013, two types of diabetes were defined by the IDF (Type 1 and Type 2). In 2023, there were three types defined: Type 1, Type 2 and gestational.
– Type 1 diabetes (T1D) is the type where the body is no longer able to make insulin (or makes so little as to be ineffective). The IDF estimates that, in 2022, there were approximately 9 million people with T1D; 1.5 million of these under the age of 20. That’s interesting because T1D used to be called “juvenile diabetes”, since it tended to appear in childhood. It is now occurring in older people more frequently. People with T1D must take insulin regularly or they will die. T1D is an auto-immune condition. We still don’t know exactly what causes it.
– Type 2 diabetes (T2D) is the type where the body cannot make good use of the insulin it produces. The 2023 definition of T2D included the phrase “insulin resistance.” This was presented as “the primary indicator of T2D.” The definition continued – “because insulin cannot work properly, blood glucose levels keep rising, releasing more insulin. Unfortunately, for some people with type 2 diabetes, this can eventually exhaust the pancreas. As a result, the body produces less and less insulin, causing even higher blood glucose levels (hyperglycaemia).”

T2D is by far the most common form – accounting for over 90% of all diabetes. This used to be called “maturity onset” diabetes, as it tended to arise only in older people. It is now being diagnosed in younger adults and even children and adolescents, which is deeply troubling.
– The new definition of Gestational diabetes mellitus (GDM) is high blood sugar that develops during pregnancy and usually disappears after birth. “During pregnancy, the placenta produces hormones that can interfere with the body’s ability to use insulin effectively. This is known as insulin resistance, a normal part of pregnancy. However, in some women, insulin resistance becomes too high, leading to gestational diabetes.”
The IDF estimated that, in 2021, approximately 21 million live births (16.7% of births) involved some form of high glucose (hyperglycaemia) during pregnancy. This is serious for both mother and baby. It can lead to pregnancy-related, and possible long-term, complications. During pregnancy, complications can include high blood pressure, large birth weight babies and obstructed labour. Longer term, babies exposed to high blood sugar levels during pregnancy may be at higher risk of becoming overweight or obese and developing T2D. The IDF reported that women who experience GDM have an increased risk of developing T2D within 5 to 10 years of delivery.
All three types of diabetes can be improved/better managed with lifestyle interventions. Richard K. Bernstein’s brilliant book “Diabetes Solution” explains how T1D can be optimally managed with a very low carb diet, and with careful meal and exercise timing (Ref 4). Dr Bernstein was diagnosed with T1D in 1946 at the age of 12. In 1969, after following ADA guidelines for more than 20 years, Dr Bernstein had many of the debilitating complications of T1D. As an engineer, he decided to examine the condition. He obtained one of the early blood glucose meters and became the first diabetic to monitor his own blood sugars. After considerable trial and error, not to mention research, he discovered that he could normalise his blood glucose through diet, exercise and medication – and that he could help others do the same. He was ignored by the medical community, of course. In his mid-forties, he decided to leave his successful career in business and go to medical school.
T2D can be put into remission with diet and exercise (predominantly diet). GDM can largely be avoided by managing blood glucose levels during pregnancy. Reaching a healthy weight before pregnancy would also help to avoid GDM.
The incidence of diabetes
The 2013 World Diabetes Day post noted “The IDF also informs us that more than 371million people have diabetes.” The same web site today reports that there are 537 million people with diabetes (Ref 5). There were an estimated 6.7 million deaths from diabetes in 2021. The IDF forecasts that there will be 643 million people with diabetes in 2030. Worse, “By 2045, IDF projections show that 1 in 8 adults, approximately 783 million, will be living with diabetes, an increase of 46%” (Ref 6). That’s a shocking indictment of our ability to improve this condition.
Because the vast majority of diabetes is T2D, the IDF reported that the key contributors to the rise in T2D include urbanisation; an ageing population; decreasing levels of physical activity and increasing overweight and obesity prevalence.
I disagree with this. Given the definition of diabetes in the opening – when insulin can no longer manage glucose blood levels – it makes sense to see diabetes as a condition of glucose handling. If the issue is handling glucose, then glucose must be a key contributor to the condition. Consequently restricting the body’s requirement to handle glucose becomes a solution. The definition told us where glucose comes from “The body breaks down all carbohydrate foods into glucose in the blood.” Hence to manage, reverse (T2D) or avoid diabetes (T2D & GDM) carbohydrates should be restricted.
I cannot understand why people who work in the field of diabetes cannot see that glucose/carbohydrates are the crux of the problem and hence glucose/carbohydrates are the crux of the solution. (Overweight and obesity may just be markers of carbohydrate intake.)
The recommendations – IDF
Much research has been done in the field of T2D especially since 2013 (Ref 7). This has culminated in there being two proposed dietary routes to manage T2D. One is a very low calorie plan; the other is a very low carbohydrate plan.
The IDF recommendation for a healthier diet is as follows (Ref 8): (I’ve put my comments along side in brackets, starting with ZH).
– Choose water, coffee or tea instead of fruit juice, soda, or other sugar-sweetened beverages. (ZH – I agree, but coffee and tea should be specified as without sugar. They should also be without milk, if being consumed between meals. Otherwise, this is grazing).
– Eat at least three servings of vegetables every day, including green leafy vegetables. (ZH – there is no benefit to T2D from eating vegetables. There’s not too much harm either – but minimums are not needed. Recommendations for vegetables should clarify “non-starchy”).
– Eat up to three servings of fresh fruit every day. (ZH – good to see an upper limit of three, but fruit is essentially sugar with a few nutrients. Fruit is best avoided for T2D, other than a few berries).
– Choose nuts, a piece of fresh fruit, or unsweetened yoghurt for a snack. (ZH – don’t snack! If you’re hungry between meals, improve your meal choices).
– Limit alcohol intake to a maximum of two standard drinks per day. (ZH – alcohol impairs the functioning of glucagon – the hormone working in partnership with insulin. Alcohol is best severely limited or avoided by anyone with diabetes) (Ref 9).
– Choose lean cuts of white meat, poultry or seafood instead of red or processed meat. (ZH – this emanates from two beliefs: i) meat is full of saturated fat; and ii) saturated fat causes heart disease. Both are false (Ref 10). Red meat contains more nutrients than white meat. Oily fish contains more nutrients than white fish, so choose red meat and oily fish).
– Choose peanut butter instead of chocolate spread or jam. (ZH – you shouldn’t need any of these because they go on bread, and you should avoid bread).
– Choose whole-grain bread, rice, or pasta instead of white bread, rice, or pasta. (ZH avoid all of these – white or whole-grain. They all break down into glucose, which people with diabetes can’t handle).
– Choose unsaturated fats (olive oil, canola oil, corn oil, or sunflower oil) instead of saturated fats (butter, ghee, animal fat, coconut oil or palm oil). (ZH – this is too ignorant to know where to start. All foods that contain fat contain all three fats. Olive oil contains more saturated fat than most meat, for example. Fat is the one macronutrient that has no impact on glucose or insulin. Any pure fat is not an issue for diabetes, therefore. People would be advised to avoid seed oils for other health reasons) (Ref 11).
The recommendations – ADA
The American Diabetes Association (ADA) is little better (Ref 12). They advise people to follow the Diabetes Plate Method (Ref 13).
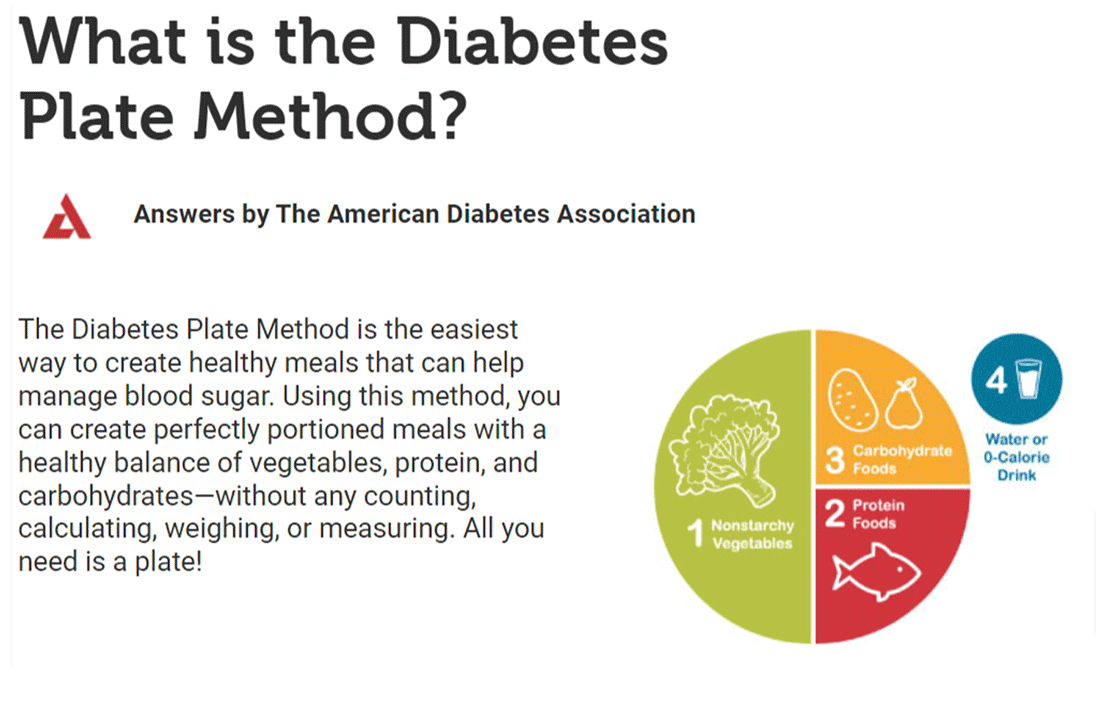
The ADA list of recommendations is shorter.
1. Fill half your plate with nonstarchy vegetables.
2. Fill one quarter of your plate with lean protein foods.
3. Fill one quarter of your plate with carbohydrate foods.
The same ignorance that we saw with the IDF recommendations about lean protein and consuming carbohydrates is repeated by the ADA. Additionally the ADA does not seem to be aware of the consequences of using a visual plate-style approach. I’ll explain, using the UK ‘Eatwell’ guide as an example.
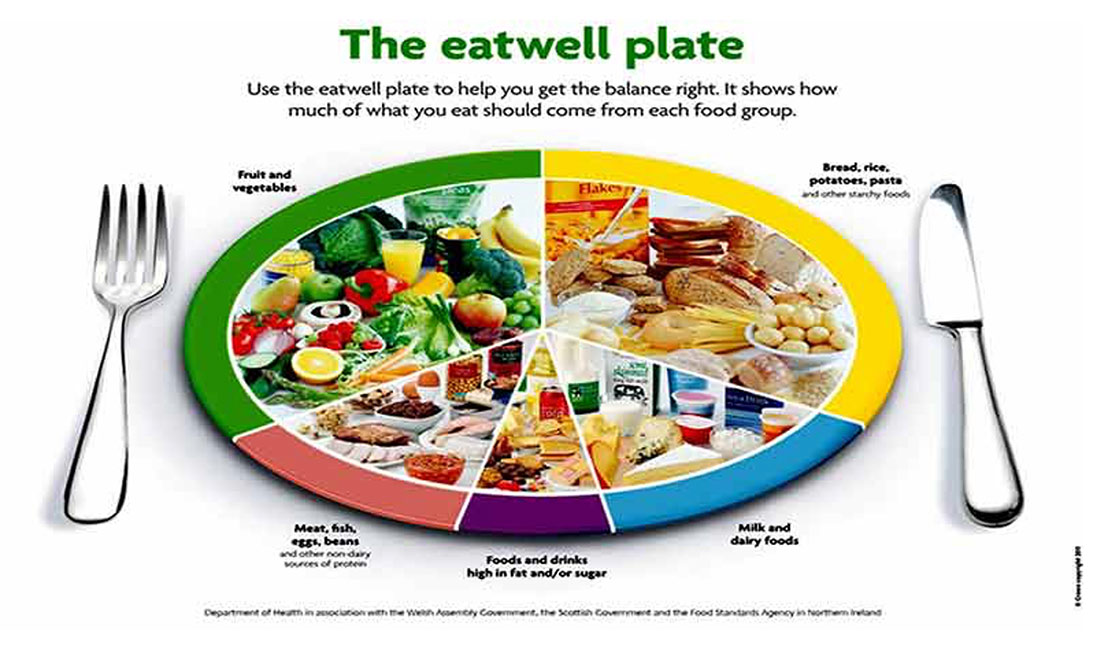
In the eatwell plate diagram, the segments represent 33% starchy foods, 33% fruit and vegetables, 15% milk and dairy, 12% non-dairy protein and 8% junk. (Rounding errors). In my 2009 book, The Obesity Epidemic, I wrote to the custodians of the UK ‘Eatwell’ Plate and asked what the plate proportions were based on. They replied “weight.” (When ones’ plate is “one third this”, “one quarter that”, yes, it’s visual but these portions will have a weight and that’s the desired outcome).
I took the average calorie number for each segment to calculate what the plate would look like if the proportions were represented by calorie intake. Calorie intake is what matters to the body and calorie intake is used in dietary studies.
A savvy calorie counter would be able to do a back of the envelope: fruit and veg is approximately 40 calories per 100g; bread is approximately 260 cals per 100g, grains are approximately 360 – starchy things will average out therefore; oils are approximately 880 cals per 100g, spreads lower – that will average too. I have a database of foods to which I commonly refer, so I worked it out more scientifically. The precision doesn’t matter much (Ref 14).
The outcome of this exercise was that the 33% starchy foods ended up as 50% of calorie intake. The same 33% fruit and veg segment ended up just 6% of calorie intake. Milk and dairy formed 12% of calorie intake and non-dairy protein was 10%. Junk – foods high in fat and/or sugar – became 22% – over one fifth of calorie intake.
The same will happen with the ADA plate. The non starchy vegetables will make up the minority of calories – probably barely 10% of calories. The lean protein will end up not far from its visual quarter. Most calories will come from carbohydrate foods. As the IDF definition knows, “The body breaks down all carbohydrate foods into glucose in the blood.”
Where we are 10 years on
We set out to review where we are 10 years on. The definition of diabetes has barely changed. It is known that diabetes is an inability to handle glucose effectively and that glucose comes from carbohydrate foods. It is admitted that incidence of diabetes continues to rise, deaths from the condition are numerous, and forecasts are for all of this to continue.
Having admitted what is known, the dietary advice is criminal. To advise such high consumption of carbohydrate when it is known that glucose comes from carbohydrates is criminal. It is killing people. The dietary advice has not even been updated to accommodate proven interventions. As a minimum, the advice should now be – choose very low calorie or very low carbohydrate. It should not be ‘consume carbohydrates, consume fruit and vegetables (more carbohydrates) and avoid fat (which drives carbohydrates to be a greater proportion of intake).’
The reason for this bad advice is why I chose my PhD topic. It has long been believed that fat causes heart disease and therefore fat must be avoided (Ref 15). As I explained in this short presentation at the UK parliament in February 2019, there are only three things (macronutrients) that we eat. We know them as protein, carbohydrate and fat. Protein tends to be a fairly constant 15% of diets. Hence any restriction put on fat necessarily increases carbohydrate as a proportion of the diet. When dietary guidelines were set to limit fat intake to no more than 30% of calories, this necessarily meant that at least 55% of calories would come from carbohydrate. We did not know if this would be safe, let alone healthy. It was merely the consequence of the dietary fat phobia.
It is this phobia today that continues to obstruct progress in diabetes. Despite my PhD showing that there was no evidence to justify the dietary fat guidelines (total fat or saturated fat) at the time they were introduced or since, these guidelines prevail (Ref 16). They are reinforced in every re-issue of the Dietary Guidelines for Americans.
The dietary fat guidelines are the single biggest obstacle to progress in the field of diabetes. Until we stop fearing fat, carbohydrate will inevitably form too great a proportion of the diet. And as diabetes organisations know, carbohydrate breaks down into glucose, which is the issue with diabetes. Diabetes doesn’t just need better dietary guidelines; it needs a paradigm shift in beliefs.

References
Ref 1: https://www.zoeharcombe.com/2013/11/world-diabetes-day/
https://www.zoeharcombe.com/2015/11/world-diabetes-day-november-14th-2015/
https://www.zoeharcombe.com/2017/11/world-diabetes-day-2/
https://www.zoeharcombe.com/2018/11/world-diabetes-day-3/
https://www.zoeharcombe.com/2019/11/progress-since-the-last-world-diabetes-day/
https://www.zoeharcombe.com/2022/11/diabetes-unpacked/
Ref 2: https://www.zoeharcombe.com/2013/11/world-diabetes-day/
Ref 3: https://idf.org/about-diabetes/what-is-diabetes/
Ref 4: https://www.youtube.com/watch?v=mkj4UQZGC3I
Ref 5: https://idf.org/about-diabetes/what-is-diabetes/
Ref 6: https://idf.org/about-diabetes/diabetes-facts-figures/
Ref 7: https://www.zoeharcombe.com/2017/12/reversing-diabetes-type-2/
https://www.zoeharcombe.com/2020/09/low-calorie-vs-low-carbohydrate-for-t2d-remission-direct-vs-virta/
https://www.zoeharcombe.com/2020/09/soups-shakes-for-type-2-diabetes/
Ref 8: https://idf.org/about-diabetes/diabetes-prevention/
Ref 9: https://www.zoeharcombe.com/2019/07/how-alcohol-affects-weight/
Ref 10: https://www.zoeharcombe.com/2023/05/the-best-rebuttals-for-nutritional-myths/
Ref 11: Chris Knobbe research https://www.youtube.com/watch?v=7kGnfXXIKZM
David Gillespie research https://davidgillespie.org/portfolio/toxic-oil/
Ref 12: https://diabetes.org/food-nutrition/eating-healthy
Ref 13: https://www.diabetesfoodhub.org/articles/what-is-the-diabetes-plate-method.html
Ref 14: https://www.zoeharcombe.com/2016/03/eatwell-guide/
Ref 15: https://www.zoeharcombe.com/2019/03/the-all-party-parliamentary-group-for-type-2-diabetes/
Ref 16: https://www.zoeharcombe.com/phd-thesis/



IDF Partners https://idf.org/our-network/our-partners/ are all pharma companies who profit from insulin, bg testing and drugs which treat symptoms. For whom low-carb diets would erode profits.
An enterprise built on a humungous pile of amputated limbs and a 14-year loss of life for the afflicted which advocates carbs for diabetics.
What a surprise!
Hi Jonty
Many thanks for this. I normally note conflicts so thank you for adding these.
Sadly yes – they are rarely a surprise!
Best wishes – Zoe
It would be much more useful if we threw out the WHO criteria for diabetes, which are based on serum glucose levels, either fasting, or in response to a measured glucose load, as in the glucose tolerance test, and lately on serum levels of glycosylayed haemoglobin, or HbA1c, and moved instead to one based on insulin levels. Thus type 1 diabetics would record a low or absent insulin level, and clearly would need insulin to stay alive, and are correctly called insulin deficient.
Meanwhile, type 2 diabetics would have raised fasting insulin, or failing that, an exaggerated insulin response curve during a glucose tolerance test, illustrating that these patients have raised insulin levels, or hyperinsulinaemia, clearly a different animal from those with type 1 diabetes. The fact that they still get raised blood sugars is a feature of their insulin resistance, and shows why it makes no sense to pile on more insulin, which in the short term gets the blood sugar down, without addressing the underlying problem of insulin resistance.
This definition would also include a submerged iceberg amount of people that would be missed by screening for raised blood glucose/Hba1c, but still have hyperinsulinaemia and insulin resistance. This would include more than those labelled ‘pre-diabetic’ who, by definition, have abnormal, intermediate glucose levels between ‘normal’ and ‘diabetic’ by WHO definition.
This would give the opportunity for truly effective preventative medicine, by addressing the insulin resistance through real food (reduced fructose, carbs, seed oils) and reduced alcohol, with exercise, rather than the quasi preventative medicine of the healthy plate and drugs, when the blood sugars finally rise high enough to show up as ‘diabetic’ by WHO criteria.
Hi Meddyg
The researcher behind the keto to ‘Eatwell’ paper would 100% agree with you on this. Insulin, hyperinsulinemia etc are Isabella’s obsessions!
Great points as always!
Best wishes – Zoe