
Familial Hypercholesterolemia (FH)
While I was in South Africa, at the Professor Tim Noakes hearing, Familial Hypercholesterolemia (FH) came up both home and away. Back in the UK, a study was published by the Queen Mary University of London arguing that public health agencies should routinely test the cholesterol levels of infants (aged one to two years) alongside the administration of childhood vaccinations. The university’s article on the paper can be seen here. The journal paper can be seen here – not on open view, but I’ve got the full PDF.
At the Noakes hearing, FH was raised by the prosecution as an argument as to why cholesterol is harmful. The argument goes – people with FH have higher heart disease and high cholesterol and therefore high cholesterol causes heart disease. (At the risk of closing the debate before having it, Dr Malcolm Kendrick dismisses this logic as follows: People who smoke have higher lung cancer and yellow fingers. Do yellow fingers cause lung cancer?!)
Let’s unpack the very interesting condition that is Familial Hypercholesterolemia (FH)…
Lipoproteins
We need a basic lesson in lipoproteins to understand Familial Hypercholesterolemia (FH).
Lipoproteins are microscopic bodies found in our blood stream. We can think of lipoproteins as tiny ‘taxi cabs’ travelling round the blood stream acting as transporters. They are needed because the vital substances fat and cholesterol are not water soluble, so they cannot exist freely in blood. The lipoproteins, therefore, carry fat and cholesterol around the body to perform their critical tasks.
There are five different lipoproteins. The largest lipoproteins are called chylomicrons. It would be logical for them to be called extremely low density lipoproteins (ELDL’s), but they aren’t. The next largest are very low density lipoproteins (VLDL’s), which are often called triglycerides, also somewhat unhelpfully. There is a lipoprotein called intermediate density lipoprotein (IDL), which you’ve probably never heard of. Then we have the much more widely known low density lipoprotein (LDL), erroneously known as ‘bad’ cholesterol and high density lipoprotein (HDL), equally erroneously known as ’good’ cholesterol.
If one chylomicron lipoprotein were the size of a football, then one VLDL would be about the size of a large orange, one IDL would be about the size of an apricot, one LDL about the size of a plum and one HDL about the size of a small grape. You can see where the notion of density comes from – the smaller the lipoprotein, the more dense/tightly packed the contents and hence the smallest lipoprotein (HDL) is high density and the largest lipoprotein (chylomicron) is the one that should, logically, be called extremely low density lipoprotein. (Ref 1)
Familial Hypercholesterolemia (FH)
FH is a genetic condition caused by a gene defect on chromosome 19. The defect impairs the body’s ability to remove low density lipoproteins (LDL) from the blood stream, resulting in consistently high levels of LDL. There are two types of FH: Heterozygous FH is found in 1 in 500 people; Homozygous FH is much rarer, occurring in 1 in a million births. (Ref 1)
Human cells have LDL receptors, so that they can receive LDLs from the blood stream and let them into the cell with all the vital lipids that they contain. With Heterozygous FH, the LDL receptor works to a slight extent and some vital lipids will get through to the cell. With Homozygous FH, the LDL receptor doesn’t work at all and so the cell doesn’t get the lipids that it needs.
Please keep in mind from the outset how rare even the milder form of FH is – 1 in 500 people. Judging from the comments on my blogs, however, you would think that maybe 1 in 10 people have FH – some doctors are clearly telling people that they have FH simply because they have a higher than average blood cholesterol level. (PCSK9s are currently only approved in the UK for FH – I suspect this is why more and more people are being told that they have FH). My first tip to anyone told they have FH, therefore, is to have a proper genetic test for the condition – a cholesterol level of 9, for example, is quite normal as defined by the normal distribution. A genetic chromosome defect is something quite distinct.
The classic view of FH
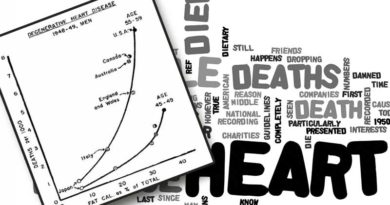
The classic view of FH is framed by the widespread assumption that blood cholesterol levels are a marker of heart disease. As this post shows, there is a relationship between blood cholesterol levels and all-cause mortality and cardiovascular disease (CVD) mortality – in men and women – but it is inverse i.e. the higher the cholesterol level, the lower the death rate and the lower the cholesterol level, the higher the death rate. That’s for 192 countries for which the World Health Organisation (WHO) has data. That’s a slightly inconvenient truth.
The classic view of FH argues that people with FH have higher heart disease and high cholesterol and therefore high cholesterol causes heart disease. Does the evidence support this view?
Because of the rarity of FH, data are not abundant. Most data emanate from the Simon Broome Register Group, which started to study patients with Heterozygous FH (the 1 in 500 form) in 1980. (The Simon Broome Register Group has been funded by Astra Zeneca, Pfizer and Merck Sharpe and Dohme, by the way).
One of the first publications from the Simon Broome Register Group dates back to 1991. This review analysed standardised mortality ratios (SMR) for 282 men and 244 women aged 20-74 with Heterozygous FH. The participants were followed up for 2,234 person years. The results were that the highest SMRs, relative to the non-FH population, were for the age group 20-39 and the higher death rates for FH sufferers decreased significantly with age, such that mortality was no higher for people aged 60-74 with FH than for people of the same age without FH.
This widely referenced study also derived from the Simon Broome Register Group. It followed 2,871 patients with Heterozygous FH who were recruited from 21 outpatient lipid clinics in the UK from 1980 to 1998. The patients were followed for 22,992 person years. The standardised mortality ratio (SMR) was calculated for these patients and compared with death rates in the non-FH population in England and Wales. There were 169 deaths recorded, including 102 from coronary heart disease (CHD) and 32 from cancer. The SMR for CHD was 2.5 times higher for the FH sufferers than the general population, but the all-cause death rate was no higher. Non-CHD mortality was significantly lower in men and women. The study found that patients with Heterozygous FH were dying more of CHD, but less from cancer and thus the death rate was no higher overall.
The combined findings from these two Simon Broome Register Group papers show that, if you genuinely have FH and you are aged 60 or over you should be pleased to know that you have a lower risk of cancer and no greater risk of heart disease. If you have FH and are aged 39 or higher, you are already past the highest risk period of your life for heart disease. Even in the 20-39 age group, there were 6 deaths in 774 person years studied – less than a 1 in 100 incident rate and that’s in 1 in 500 people.
Another widely referenced, long, Dutch, study set out to estimate all-cause mortality from untreated FH. The study was described as a “Family Tree Mortality Study”. It traced back numerous descendents from a single pair of ancestors in the 19th century. Those with a probability of carrying the FH mutation were followed. This involved 250 people analysed for 6,950 person years during which time 70 deaths occurred. The study found that mortality was no higher in carriers of the FH mutation during the 19th and early 20th century. Mortality rose after 1915, peaked between 1935 and 1964 and fell thereafter. Mortality also differed significantly between the branches of the descendents studied. The conclusion was that the risk of death differed too much over time, and too much between different descendents, to support the view that high cholesterol was the factor. The study concluded that environmental factors must play a part and must be researched more thoroughly. Sadly this has not happened, because the cholesterol hypothesis has become the only factor considered important with FH.
An alternative view of FH
If you are not limited by the assumption that high cholesterol is bad, you can view FH quite differently.
My logical consideration of FH suggests to me that the problem is that the LDL receptors don’t work properly and therefore LDLs cannot get into the body’s cells in the way that they are supposed to. This means that cells don’t get the vital LDL, carrying the vital protein, lipids and cholesterol needed for the cell’s health. LDL in the blood stream is high because the LDL has stayed in the blood stream and has not been able to get into the cells – where it is supposed to go. Hence high LDL blood levels are the sign that someone has FH. The high LDL levels are, however, a symptom and not a cause, or a problem per se. The problem is that the health of every cell is compromised by LDL not getting into those cells. This includes heart, brain and muscle cells – all cells. Someone with FH can therefore have heart problems – because of too little LDL reaching the heart cells – not because of too much LDL in the blood stream. How differently things can be seen when one is not blinded by thinking that cholesterol or lipoproteins are bad.
The heart disease/cancer evidence supports this hypothesis. If the vital substances in LDL cannot get to heart cells, heart disease would be more likely. If the vital substances in LDL cannot get into a cell that has become cancerous, that cell can’t be fed and the cancer is less likely to spread.
A genetic view of FH
There are also alternative hypotheses for FH involving genetics more broadly. These make complete sense. This article, cited almost 50 times, studied 1,940 FH patients for 65 polymorphisms (different forms) in 36 different genes and found a significant association between “Prothrombin G20210A” and CVD risk. Don’t worry about the unfamiliar words – all we need to know is that Prothrombin G20210A is a human gene mutation that increases the risk of blood clots. The study found, therefore, that people with FH who had an accompanying genetic mutation that increased blood clots were more likely to suffer CVD. That makes sense, of course. It also makes sense that a genetic defect, which is what FH is, has more than one consequence. Another genetic consequence of FH (completely unrelated to cholesterol) can be increasing the risk of heart disease (and the same genetic consequence or a different one may be reducing the risk of cancer). The raised LDL would, again, be a symptom and not a cause of heart disease in any way.
What about statins?
You may be interested to know that there are no intervention studies that directly show mortality benefit of cholesterol lowering in FH. Despite this, because of the limiting belief that cholesterol is the problem (and not the symptom), all treatment for FH focuses on lowering cholesterol. Statins are administered. Bile acid sequestrants are used (e.g. cholestramine). Ezetimibe might also be used, which inhibits cholesterol absorption in the gut. Anything and everything that can lower cholesterol is considered part of the toolkit. No benefit has been established in doing this and yet the Queen Mary university article, recommending routine cholesterol testing of infants, proposes that statin ‘therapy’ can start earlier. This recommendation could lead to children being put on statins and other cholesterol lowering medication during their most formative years when we know that cholesterol is a vital component in cell and human development. A clearer case of child abuse would be difficult to find. (The lead author of this infant/statin paper, David Wald, is the founder and shareholder of Polypill Ltd – a four in one drug, which includes a statin).
If raised LDL is a symptom and not the problem, any cholesterol lowering medication would only make things worse. If LDL not getting to cells is the real harm of FH, then any attempts to lower cholesterol will make things worse. We know from the brilliant book by the Yosephs that cells will try to produce cholesterol if they cannot get it from the blood stream. We also know that brain cells produce cholesterol because of the blood brain barrier (which is why statins can have particularly harmful effects to mind, memory and mood). If people with FH are already suffering from LDL not getting to cells, then impairing the cell’s ability to make cholesterol will make things even worse.
People with FH should ideally be given medication (if anything existed) to stimulate cholesterol production within the cell, so that the cell would at least get the vital cholesterol it needs, even when it couldn’t get it from the blood stream.
How differently problems can be viewed when unconstrained by limiting beliefs.

p.s. if you would like to see the Dr Malcolm Kendrick yellow finger hypothesis and a five minute take down of FH, watch this from 15-20 mins.
Ref 1: Mangiapane EH, Salter AM. Diet, Lipoproteins, and Coronary Heart Disease: A Biochemical Perspective: Nottingham University Press 1999 January 1, 1999.


HI Zoë,
Appreciate all the work you are doing.
I have been FH diagnosed in 2016. Through genetic testing. Heterozygous.
With the following numbers pre statin: Total: 14.4; HDL: 1.8; LDL: 12.2; Trig: 0.84 (Only from age 28/29 really, before that pretty “normal”). I am 38 Now.
On statin: Total: 4.04; HDL: 1.27; LDL: 2.36; Trig: 0.9.
I am on zuvamor(40mg) and ezetrol(10mg).
Why am I taking away, the very thing that my body needs!? The more I read about Cholesterol the more I question the need for medication. Or at least the levels I am currently on. I am 38, Fit, recently started LCHF lifestyle. And intermittent fast 16/8. Live in Gauteng, South-Africa.
So in my mind, IF CVD is the biggest risk for someone with FH (which according to what I read and saw so far is not entirely true!), surely one should look at the whole picture. Lifestyle, condition of arteries etc? And especially if arteries are in good condition, I have no need to be on statin?
To top it all, my profession requires my CVD risk to be low/managed. And the medical board sees high cholesterol as high risk. Unless you can prove other risk factors are normal.
What advise/guidance can you perhaps give me? Or perhaps a referral to a dr/cardiologist in SA that will be willing to walk this journey with me with an open mind regarding cholesterol. I am responsible for my own health, and do not want to be reckless or irresponsible.
Best regards,
Petrus Pienaar.
Hi Petrus
I can’t give advice – just information. Your case is really interesting as I’ve not seen such low cholesterol results for someone with confirmed FH on statins. Quite often people still have high total and LDL cholesterol even on statins. 4 and 2.3 is low!
You may find the work of Dr David Diamond interesting. He asks the right question in my view – if FH/high cholesterol is so deadly, why does everyone with FH not die prematurely? He asked what is different about those who die early (https://www.zoeharcombe.com/2020/02/the-british-heart-foundation-and-familial-hypercholesterolemia/)
I do think that the whole health picture should be taken into account. The work of Kraft – shared often by Dr Jeff Gerber and Ivor Cummins is very interesting too – on calcification and coronary calcium scores. They have videos on line if you search their names and those terms.
You’ve got a number of thought leaders in South Africa (like Prof Tim Noakes) who are interested in this area, but I don’t know of any practising medics in the heart field in SA unfortunately. Here’s a long video from the prof! https://www.youtube.com/watch?v=jyzkv5uFGt8
You’re already doing LCHF and fasting – that’s the arena where you’re likely to find a doctor/cardiologist who is open minded on the cholesterol/diet subject. I hope you find someone through this route.
Best wishes – Zoe
Thank you.
Appreciate the information.
Hello Dr. Zoë Harcombe
It is now 2021
1 – do you still have the same beliefs that positive FH people do not need statins?
2 – can a positive FH person live a life free of heart disease with very high cholesterol numbers as long as they choose a healthy lifestyle? (For example, eat healthy, meditate, exercise, be mindful, spend time with family and friends.)
Hi Meeshelly
I’m an academic doctor not a medical doctor – I don’t give advice.
Hence 1) please tell me where I have ever said that positive FH people do not need statins?
2) no one can know the answer to this question for a person with confirmed FH anymore than any other person. I live an extremely healthy lifestyle and I cannot guarantee that I won’t get heart disease. With the current stress of the world losing its mind I am becoming a more likely candidate for heart disease by the day!
Best wishes – Zoe
Just reading through some of your posts plus those from other people and this is all fascinating.
I am 66, I exercise for around 1hr daily – walking, Qigong and Zumba
BMI is 21.9
BP (after 24hrs on a monitor) is 14/90
cholesterol is
Total: 7.9 HDL 2.26 LDL 5.1 Tri 1.43 Ratio Total/HDL 3.66
Diet and exercise make no difference to my levels. Before I was put on Prolia for bone density my cholesterol total was always about 1.0 lower than this. I have reads Prolia can raise cholesterol. I have tried plant sterols, high strength fish oils and more recently Lipantil. I have come off all of them within a week (lasted 4 days on lapantil) as with all my muscles start to ache which leads me to believe my body needs this cholesterol and objects if I try to lower it.
I have just been put on Ramitace for blood pressure.
My Dr is lovely and I can talk to him about all of this but what I am wondering now is should I be trying to adjust my diet again (cheese, veg, fish, fruit, little meat at the moment) or am I better getting my heart checked over or is there something else I should be asking about?
My maternal grandmother had two strokes and my mother had high blood pressure but I know no more than this.
Thanks
Prioritize meat & eggs. Veg is not necessary & fruit should be minimized.
My dad died last year of a heart attack and he was pretty healthy I’d say. I was advised to get my bloods checked and the results are below.
Fasting cholesterol 7.2
HDL Cholesterol 2.0
LDL cholesterol 4.2
Non HDL Cholesterol 5.2
I’m healthy , fit , non-smoker and on the skinny side but I was told to think about my diet and they’re now checking for FH. I’m now worried? I don’t understand any of the levels but I also don’t really relish the thought of a plant diet???
Any ideas?
Hi Maya
I’m sorry to hear about your dad. I don’t know how old he was but the major factors with heart disease and death are age, sex and genetics (https://www.zoeharcombe.com/2014/05/heart-disease-the-facts/)
Your cholesterol tests do not suggest FH at all. FH levels tend to be in double figures – sometimes even when on statins. I think that FH should always be diagnosed properly (i.e. do you have the genetic condition) Not just because cholesterol is high. Yours isn’t even that high – it would have been pretty normal in a pre statin world (https://www.zoeharcombe.com/2014/06/diabetes-cholesterol-bp-normal-is-no-longer-normal/)
This might be of interest too (https://www.zoeharcombe.com/2015/03/worried-about-cholesterol-andor-statins/)
I can’t advise. I can say that those results wouldn’t worry me personally for on second.
Best wishes – Zoe
This article has really been helpful. I’ve been LCHF since Oct 2017. My LDL readings have remained at similar levels pre LCHF and present between 4.6 and 4.8. My GP of course concerned despite my Trig to HDL ratio being 0.6 and seeing vast improvements in these readings. My mother was “diagnosed” with FH and lived to 81 died of stomach cancer, smoked most of her life. I am concerned I have FH. Your article has put my mind at ease to continue with LCHF and avoid statins. How is FH diagnosed and is it really useful as I’m convinced my GP will just push statins? My father died of CVD at age 64 and his mother also in early 60’s from angina. I am fearful of my fate and wish to do the best to prolong my life.
Hi Megan
I’m sorry that your father and his mother died so young. Your mum is a good guide though, so let’s hope you have more of her genes.
FH should be diagnosed with a genetic test because it is a genetic condition – as explained in the article. However, far too many doctors diagnose it on the basis of a cholesterol reading alone. In a normal distribution, some people will have a total chol of 2-3 and some will have 9-10. That’s what the normal distribution means. However, those at the top end are increasingly told they have FH and quite frankly they don’t.
I personally would insist on a genetic test before accepting anyone telling me I had FH.
Best wishes – Zoe
Zoë, hello. I am benefitting from reading through this thread: have you an idea where/how I/we could get the genetic test for FH. I was told after an overnight TIA stay in hospital that I had it. I’ve not had satisfactory recommendation regarding results a friend got from 123… I’m in Ireland/uk.
Hi Julie-Anne
I’m sorry but I don’t know where you can get genetic tests for FH. Hopefully your medical team can help you.
The cholesterol level alone is often taken as diagnosis, but it’s a genetic condition that would ideally be confirmed as such.
I hope you find an option.
Best wishes – Zoe
was diagnosed with familial hypercholesterolemia. I have ehlers danlos also
Total Cholestrol 8.8
LDL 7.0
Non HDL 6.2
HDL 1.5
TRIG 1.7
Doc trying to put me on statins i dont know what to do
Hi David
I can’t give any views on what any individual should do. That’s between you and your doctor. I can just provide information.
I wonder if you’ve been diagnosed with FH properly? i.e. with a genetic test? or from your cholesterol level? because the latter is not that high. In pre-statin eras, that would have been seen as a bit above normal.
That’s my only observation
Best wishes – Zoe
Thanks for reply. Just noticed your reply unfortunately.
I was diagnosed with FH purely based on cholesterol levels and family history.
Granda – 3 heart attacks. Age 50, 52 and 56.
Grandad 2 3 heart attacks. Age 50,55 & 58.
Dad triple bypass age 58
Grandma – died vascular disease age 45.
I expirmented once with plant based diet and got my normal to level for the first time ever. I’m 40 years old. I did however feel better with animal products in my diet.
Anyway my levels have increased again slightly and doc pushing statins.
I know you can’t tell me what to do but due to family history and my Ehlers-Danlos (chronic fatigue and pain I can’t exercise at all) I have been worrying about my cholesterol and family history.
Hi David
As I shared previously – I can give information and opinion, but not advice.
I’m really sorry to hear about this family history. I would ask for a genetic test to confirm FH – the reading you shared previously (8 not on statins) is not obviously FH territory. Were there any other factors that could reassure you that you are different to your relatives? Smoking? Obesity? Workplace? I would also be working with the medics to explore all reasons for family related heart disease. Is it cardiomyopathy?
This may be of interest – even among people with FH, there is a difference between those who have an event and those who don’t and understanding that is key. (https://www.zoeharcombe.com/2020/02/the-british-heart-foundation-and-familial-hypercholesterolemia/)
This is why a plant based diet (high in plant sterols) would lower cholesterol, but my research found that it’s not good news for heart disease (https://thescipub.com/abstract/10.3844/ojbsci.2014.167.169).
I hope this helps with a couple of avenues to explore with your consultant(s)
Best wishes – Zoe
Thanks again for reply and information.
Both grandads dud smoke for around 15 years and stress.
Can I ask you one more question I have a creased earlobe and I’m reading this is also a risk have you any idea on this? Maybe the crease is due to my connective tissue disease.
The last 5 years of my life have been extremely stressful due to my chronic illness losing my job health home wife etc. It’s no surprise if I am at risk after this trauma and now 40 years old
Hi David
I would take some reassurance that smoking is a different factor for you and an important one.
I’m really sorry to hear of the stress you’ve been through. Stress is a risk factor for heart disease and not good for healthy generally so – I know easier said than done – but any stress management you can do will be worthwhile (meditation, yoga, walking, time in nature, time doing things you enjoy, laughing etc) The stress factor has been exacerbated in so many people over the past year, as the normal outlets for stress (social contact and fun) have been obliterated :-(
I have never researched the creased earlobe issue so I am unable to comment on this sadly.
Best wishes – Zoe
Hi Zoe.
I found this article very interesting, thank you. I have a question but maybe it is silly, I’m not sure. It’s my understanding that there is a belief that heart disease is caused by blood clots rather than high cholesterol, therefore would people with FH not benefit from an aspirin rather than a statin? Is this too simplistic?
Thanking you.
Claire Fitzpatrick
Hi Claire
Thankyou! And there’s no such thing as a silly question in science! And this one certainly isn’t silly.
This presentation may be of much interest. It’s Dr David Diamond talking about clotting as a risk factor in FH (https://www.crossfit.com/essentials/david-diamond-ldl-lies-health-conference-video) I think he gets to the clotting bit within the first 20 mins but don’t hold me to it!
Aspirin is taken (low dose) as an anti-clotting agent. There are also stronger anti-clotting agents and yes I do think this should be explored more than it is. And David would more than agree no doubt.
I hope this helps
Best wishes – Zoe
p.s. our recent paper may also be of interest https://ebm.bmj.com/content/ebmed/early/2020/07/05/bmjebm-2020-111412.full.pdf
Hi Zoe,
I can’t thank you enough for this informative article!
My cholesterol total is now 360, I’m 60, and have to date refused to take a statin…. due to family history….
Most on my mother’s side have cholesterol in the mid 3’s, aunts, uncles and cousins. We’ve not been genetically tested for FH. My mother and her five siblings lived well into their 80’s, some 90’s, with not one incidence of heart disease and without being on a statin.
When I read articles like this, it bolsters my confidence that I’ve chosen the right path, less meds, healthy diet, stress reduction and exercise.
(I typically start to re-research just prior to “the checkup”, lol, where statins will be pushed and the dance with (condemnation from) the doctor begins. It is why my checkups are far and few between.
Kim
Hi Kim
Many thanks for your kind words. I’ve just returned from a huge heart conference where there was a brilliant presentation on FH. I’ve just emailed the speaker to see if it it on open view anywhere. If it is, I’ll add it to this reply – fingers crossed!
The gist of it was that – among people with FH – a few people die early (of heart disease), but most don’t. The speaker, Dr David Diamond, took the approach – all the FH people have high cholesterol and yet some die early and some don’t. What else is different between those who die early and those who don’t, because it isn’t cholesterol (because the cholesterol is equally high in all of them). He found that people with FH are particularly susceptible to smoking and stress and a couple of other things and therefore it is even more imperative for people with FH to manage certain lifestyle factors. However, they are not told this – they are just told to lower cholesterol – which is not the differentiator!
Best wishes – Zoe
p.s. try this at about 35 mins in: https://www.youtube.com/watch?v=psnkNqLA4Os
Fantastic article Zoe!
I’m glad you can think outside the box.
Your article refers to the heterozygous version of FH. What about the homozygous version?
Thanks!
Hi John
Many thanks for your kind words :-)
The article mentions Homozygous FH (and how rare it is). I see this as a more extreme version of Heterozygous FH. The receptor doesn’t work at all, as opposed to not working well. I think that it is even more the case that the LDL in the blood stream is a marker, not a maker, of a problem. The problem is the cells not getting the goodies in the LDL taxi that are needed. In Homozygous FH, the only option for each cell is to make what it needs. Statins will impair this and – I think – do even more harm than when given to someone without FH.
Best wishes – Zoe
Thank you Zoe!
If the very high LDL in a person with Homozygous FH is not responsible for plaque build up or heart disease, does it cause other problems from being so high? I can think of the issue of Xanthomas, where excess cholesterol makes fatty deposits under the skin. Perhaps in that situation, lowering of cholesterol (even with drugs) would be warranted?
I was reading here, at the FH Foundation about treatments:
https://thefhfoundation.org/heterozygous-vs-homozygous-fh
I found it interesting that a liver transplant could normalize LDL because the new liver has a normal complement of LDL receptors. I didn’t see any info about whether or not a person would live longer and healthier after this procedure.
It also makes me wonder then if the defective LDL receptors are in the liver mostly, and less so in the cells (or maybe both)?
Hi Dr John
Sorry this one got missed being approved and answered while I was away for a week…
I don’t think that cholesterol is an issue or a cause of anything per se – it can be an indicator. High LDL with FH is an indicator of FH – as the post shares, I think the issue is the LDL not getting to the cells where it is needed – the LDL in the bloodstream is just a marker of an issue. Ditto Xanthomas are a marker to me – do they cause any harm per se? They may be unsightly – but are they a health problem?
Best wishes – Zoe
Thanks again Zoe!
A comment you made below (from Malcolm Kendrick):
Believers: “It’s small and dense vs large and fluffy cholesterol”
Malc: “When will you just shut up and admit you were wrong?!”
My current understanding is that the small dense LDL is the only “bad” cholesterol because it is what’s responsible for infiltrating the endothelial lining in the arteries and starting the inflammatory process of plaque build up. Is that totally wrong? If so, then what does cause the buildup of plaque in the arteries?
Also, does it intrigue you that a liver transplant can normalize LDL? Does that perhaps mean that the liver produces defective LDL in FH that cannot be absorbed, rather than the cells having a problem taking it in?
Hi Dr John
This is the post you need: https://drmalcolmkendrick.org/2018/08/16/what-causes-heart-disease-part-52/
I didn’t know about the liver transplant – it horrifies me more than intrigues me. The idea that we administer statins to achieve a number we made up is bad enough – that we would transplant someone’s liver is beyond comprehension.
Best wishes – Zoe
The article was very informative, thank you! Malcolm believes blood clots cause arterial plaque (not cholesterol). It wasn’t clear to me reading it though as to what causes the blood clots, and how to treat someone who has plaque buildup. Can you share what you know about this?
Hi Dr John
This is the site you need – Malcolm is up to part 54 – over 100,000 words to keep you busy!
https://drmalcolmkendrick.org/2018/08/31/what-causes-heart-disease-part-54/
Best wishes – Zoe
How come I (the non smoker, green tea, heart foundation diet follower) had a NSTEMI abd 90%heart block, triple bypass and the Cardiologist blamed genetics. My older fatter heavy smoker sister who ate crap and salt +++ never had any cardiovascular issues. We are both Registered nurses and brought up on same diet. Cholesterol is NOT familial.
I recommend Gary Taubes’s articles about fat & salt, showing the lack of science behind the recommendations. Your problems were probably caused by replacing healthy saturated fat with toxic seed oils (“vegetable” oil). Ditch the Heart Foundation Diet.
Hi Zoe
At long last reporting back on my FH genetic test. I have an average total chol (TC) of over 10.00 mmol/L and got the results today and…
…you’d have won the fiver!
I’m not FH. The NHS results letter states: “the laboratory has NOT been able to identify a gene alteration that is known to be associated with FH”.
Strangely, the letter also added “this does not change your clinical diagnosis of possible FH and therefore you should continue to have treatment for your raised cholesterol”.
Scaremongering? Or some sort of future proofing against developments in FH research? Or butt covering?
Not sure whether my high TC is my normal though:
On the one hand, no (as yet) discovered conditions which might account for high TC e.g. no thyroid and diabetes type problems and blood metrics such as lp(a), fibrinogen and homocysteine are OK.
On the other hand, I have a very high arterial calcium score indicating chronic arterial damage with the body/liver generating help molecules such as cholesterol to repair the damage.
Well, that’s the FH news and I think ties in with your views above.
Kind regards
Hi Charles
Many thanks for the update – how interesting! I suspect the letter means – we still think your body is making cholesterol because it is trying to kill you, so continue to be saved by your statins. For goodness sake!
Your view on the cholesterol likely being there to repair would get my vote. The calcium score is not good – have you seen videos by Ivor Cummins? The work of Joseph Kraft?
http://www.thefatemperor.com/blog/2015/9/5/fat-emperor-productions-present-the-kraft-interview-decoding-diabetes
(Don’t think his work is about diabetes – it’s mainly about arterial calcium and how all people with heart disease have diabetes… very interesting work.
Best wishes – Zoe
Hi Zoe
Nice summary on FH. I have a question: do we really know that cells are cholesterol deficient when half of the receptors are defective?
About 40 years ago a Dr. Hazard (real name, honestly) of the Lipid Research Centers Program told me that having half the receptors on a cell still allowed all of the lipoproteins into the cell that the cell would need. He postulated that serum lipid levels were elevated, not because the cells were not taking in enough; rather there was some mechanism associated with the receptor sites that “counted” the receptions per unit time (flow rate) and released a signal (enzyme, hormone?) back to the liver as a feedback signal. So when the number of receptor sites is half of normal, the flow through per receptor doubles, and the liver gets a signal that says the cells need more lipoprotein than they actually need. I seem to recall that he went so far as to say, in the absence of external cholesterol delivery, that cells could produce their own cholesterol. Again that is my recollection from mid-1970’s.
Hi Rob
Many thanks for this – I’m open to any explanations! The only one that doesn’t make sense to me is that the body is making cholesterol to try to kill us! ;-)
Best wishes – Zoe
P.S. Sarah
Don’t think I made the key point about LDL chol measuring, which is with very low triglycerides the standard Friedewald method overestimates LDL chol, which I hope my figures illustrated.
The abstract of the Iranian paper stated “statistical analysis showed that when triglyceride is <100 mg/dL, calculated low-density lipoprotein cholesterol (LDL) is significantly overestimated (average: 12.17 mg/dL or 0.31 mmol/L)".
Hi Sarah
Here are my 2 pennies worth…
You refer to a “family history of suspected FH” – Dr Harcombe is right: you need to get a genetic test. Here, in England, your 1st port of call is your GP.
You may also wish to read my comments elsewhere for further details: it’s the “journey” I’ve just embarked upon. I met the criteria for referral and had a consultation with a nurse from a genetics team a few weeks back. It was a hour long consultation, they go through your family history and talk about FH. And you give a blood sample and wait for the results.
I don’t know how good your (or my!) knowledge of lipids is, but they are looking at low density lipoprotein (LDL), as covered above by Dr Harcombe.
You may think when they take a blood sample for a lipid profile (or to measure LDL) they just measure what’s floating around in the sample. No – it’s calculated according to a formula devised and known as the Friedewald formula/equation. (You can get an actual LDL chol measurement but I’ve found that’s another complicated story) The Friedwald equation, I gather, is pretty accurate. Unless your triglycerides are very high. Or very low and the Freidewald equation is less accurate – the Iranians discovered that Friedewald is also inaccurate for those with very low triglycerides.
Here are my Sept 2017 measurements for illustration:
triglycerides: 0.5 mmol/L
LDL chol (Friedewald): 5.61 mmol/L
and when run through the Iranian equation my LDL chol drops to: 4.36 mmol/L.
Personally, I’m not alarmed at either of these LDL chol figures but they think I need statinating like a force fed pate foie gras goose.
So why am I getting a genetic FH test? Well the figures have been a lot higher in the past is one reason.
Hope this helps.
Oh, and I’m not a doctor or healthcare practitioner or scientist…I’m a layman/member of the public taking an interest in his own health. That’s my disclaimer!
And all of the above may not get through Dr Harcombe’s moderation anyway!
Regards
Charles Gale
I love the comment about being statinated like a face fed pate foie gras goose. Really made me laugh! Thanks – Ed
Hi just after your opinion. We have a family history of suspected fh. My grandad fit and healthy dies at 43. My mum and auntie have it. I also do and have been on and of statins since I was 15. My chlosterol is now 4.7. My daughter just got tested at 3 and a half and we are very worried as the reading came back as 8.2 she eats so well as is very active. We’ve been told not to worry and she has been referred. They said she will start statins as young as 8. Any thoughts??
Hi Sarah
There’s not much I can add beyond the post you’ve commented on. In my honest opinion, you do not have FH with a cholesterol level of 4.7. True FH, you’d most likely have double digit cholesterol on statins. Have you had FH confirmed with a genetic test?
Before any child is ever put on statins, any parent (and doc) should know what they do https://www.zoeharcombe.com/2013/10/how-statin-drugs-really-lower-cholesterol-and-kill-you-one-cell-at-a-time/
I have no idea how a human being could develop normally from child to adulthood while on statins. Growth must be impaired. Given the vital importance of cholesterol for sex hormones, you may also want to think about your daughter ever wanting children!
I’m quite horrified by the thought of a child taking these inhibitors.
Best wishes – Zoe
Hi Zoe
I thought I’d report on my FH testing journey and result…
…since August, having met the criteria, I did get a referral for a FH genetic test and met the nurse and gave a blood sample…last week! So, all that took some time but the waiting gets worse. The nurse advised the results would take…drum roll…about 3 months…i.e. early next year!
I’m in no rush and used the waiting period before the test to think about the lipid/cholesterol hypothesis and (1) thought I’d see what some trusted sources said about it (i.e. Doctors Malcolm Kendrick and Mike Eades and a few others) and general googling and (2) have a current lipid profile blood test done.
I can see the appeal of websites and blogging. I’m tempted to hijack this comment section and put down my thoughts on all this such as the 4 separate hypotheses within the lipid hypothesis/LDL: (1) some say LDL – C (2) some say LDL particles (3) some say LDL particle size and (4) some say LDL particle oxidation.
Then there’s LDL-C testing: I thought it was whatever was in the sample. Nope, it’s a Friedewald equation, which doesn’t work for high or low trigs then you need the Iranian calc, or a direct measurement.
As for the results – it’s interesting what they leave in, and what they leave out e.g. no trig/HDL ratio which some consider a good marker, LDL-C hasn’t always appeared on my results but non HDL chol does (NHS choices says because “it’s thought to be a more accurate way of estimating CVD risk than LDL”).
And what they cherry pick from the results to medicate you, and what they ignore. I can do that too.
What a carry on!
Anyway…I’ll report back.
Kind regards
Charles Gale
Hants
Hi Charles – comment away! I for one am loving it :-)
You’re showing nicely what a whole heap of nonsense this all is. Dr Malc Kendrick puts if best:
Believers: “It’s cholesterol”
Malc: “No it’s not”
Believers: “It’s good and bad cholesterol”
Malc: “There’s no such thing.”
Believers: “It’s the ratio of good and bad cholesterol”
Malc: “See previous answer.”
Believers: “It’s just bad cholesterol”
Malc Rolls eyes!
Believers: “It’s small and dense vs large and fluffy cholesterol”
Malc: “When will you just shut up and admit you were wrong?!”
Best wishes – Zoe
I’ve got FH type IIa with TC of 400, give or take. My dad died of anMI at 33 and I had the first of four at 39. I came to the conclusion about seven or eight years ago now that CVD, especially for those of us with FH, was really a form of diabetes. After running across Dr.Joseph Kraft’s research, I was convinced. I eliminated most carbohydrate from my diet and increased the fat and started to improve. My story in just a few minutes: https://youtu.be/kv1KJzgKz5U
Hi Ron
Many thanks for sharing this – we’re both Ivor and Joseph fans! Great to see how well you’re doing.
Best wishes – Zoe
Hi Zoe
Thanks for the very useful reply.
I’ve had two FH diagnoses based on high Tot Chol (TC), so enjoyed your article.
I went on the NHS website and stuck FH in their search engine. The NICE guidelines state for TC over 7.5 mmol/l the patient should be assessed and referred to a specialist assessment which may include DNA testing.
This was printed off and stuck under my GPs when he started to resisting my request for a DNA test. He double checked his system and had to agree to look into the matter.
Here’s hoping. And how nice (pun intended) for once to use NHS/NICE guidance for one’s own interest…normally, it’s the NICE guidelines they use to shut you down.
Hopefully, a DNA test will be forthcoming and use science to either confirm FH or that my high TC is my normal level.
Regards
Hi Charles
Do let me know if you have FH! I always thought you needed to have TC in double figs even on statins to be in that ball park. I’ll put a fiver on you NOT having it!
Best wishes – Zoe
Hi Zoe
I’ve followed you since last year and it was through Dr Kendrick’s website and blogs I got your details.
Could you tell me what the genetic test for FH is?
On the one hand, my total cholesterol over the years is constantly over 10 mmol/L (maxed out at 18 one year) and I have xanthelasma in one knuckle and, together, that may be sufficient for a diagnosis.
Would it even be worth requesting a test from my GP?
Would it be available on the NHS here in England?
It would be nice to know it’s not stress or fasting blood test raising the cholesterol levels.
Regards
Charles Gale
Hi Charles
FH is a genetic condition caused by a gene defect on chromosome 19, so you need a test to see if you have that defect. I don’t know how you get one – starting point for anything medical is the GP in the UK. I don’t know if it’s available on the NHS – If anyone diagnosed me as having FH without doing this test, I’d demand one!
Remember – there are highs and lows on any normal distribution – by definition. Some people have a cholesterol level of 3, some have 10 – they’re both on a normal distribution (https://www.zoeharcombe.com/2014/06/diabetes-cholesterol-bp-normal-is-no-longer-normal/) The trouble is – our powers that be have decided that the norm shall not be 7-8 – 5 shall be decreed as high! Work that one out!
Best wishes – Zoe
p.s. Uffe Ravnskov’s book Ignore the Awkward has an interesting chapter on FH
p.p.s this looks interesting https://www.lipid.org/sites/default/files/9-_knowles-genetic_testing_for_nla_v2.pdf
Hi Zoe
I’ve read a lot of your stuff and watched your presentations. Great.
My queries: erratic bp (resting = 150s/90s, briefly mega stressed = 188/103). Is this ok?
I’m doing lchf intermittent fasting and full day fasting to see how this afdects bp and rhr (70s).
Cholesterol = 13. Should I be teated for FH? Should I be concerned?
Just developed mild, but spreading psoriasis.
I’m a bit surprised as I’ve eaten RMR green list only (dedicated but veggie) for 2.5 yrs, am 54kg, 164cm, 55 yrs female, active.
You can imagine the response from the gp is! No way am I going to use meds. She ignored the psoriasis.
Your opinion, and facts would be very helpful. Also, any contacts for genuine wellness-type doctors (evidence-based only – no flakey/fluffy types!)
Best to you
J
Hi Julie
Many thanks for your kind words. Please note that I can’t give medical advice – I’m a PhD, not a medical doctor – but no medical doctor would over a blog comment (I hope!)
I can give opinion and facts and info and leads as requested…
On the BP – if you go through to the article linked in this post (https://www.zoeharcombe.com/2014/06/diabetes-cholesterol-bp-normal-is-no-longer-normal/) you’ll see that the true normal BP is about 140/90. You can then see the normal distribution of people from low to high. You are a bit above normal at 150/90 but some people are above normal and some are below – that’s how averages work! The high stress BP is not great – I’d work on understanding the sources of that and stress management – the BP is the symptom – try to fix the cause.
On the cholesterol – as the post you commented on says, FH is a genetic condition – you’d be better off getting tested for the gene and then you would know. High cholesterol per se is not a diagnosis. As you can also see from the post, if you do get a genetic diagnosis, I personally don’t think trying to impair the LDL function further is the right thing to do – that’s my view. You may like to read this too (https://www.zoeharcombe.com/2015/03/worried-about-cholesterol-andor-statins/). Check out the inaccuracy of the cholesterol test. Plus – if you live in the n hempishere and you’ve recently had the test – check out the bit on vit D and sun.
On the psoriasis – stress can also be a cause – back to stress understanding and management. Interestingly – one of the best leads for further watching/reading on that “worried about” post is Dr Malcolm Kendrick (google him). He also thinks stress is a huge factor in heart disease. Psoriasis can also indicate low immunity so you may like to check you don’t have nutrient deficiencies. The veggie bit worries me (having been there myself for 20 years) – you need 39 eggs daily to get 15mcg of vit D or c. 200g sardines. We have a nutrient checker in our on-line forum (theharcombedietclub) – there are many on line – you may like to enter what you eat on a regular basis and see if you’re missing anything. Vit E is common to be low in and vit E plays an important part in skin health. Sunflower seeds would cover this… (https://www.zoeharcombe.com/2014/04/the-perfect-five-a-day/)
Top doc I recommend to read is Dr Malcolm Kendrick. Also Dr John Briffa.
Hope this helps
Best wishes – Zoe
p.s. great job on your weight, height and activity :-)
I predict that you could cure your skin condition by eliminating plants from your diet, as Aaron McKenzie has done https://www.youtube.com/watch?v=sit9Vlt-9Pw See also Paul Saladino.
Hi Zoe
I have recently been diagnosed with PAD. I have almost 100% blocked artery in my right leg and around 50% in my left. I have suffered with my legs fatiguing very easily for sometime without it being diagnosed which is mainly because claudication generally only happens when you’re a lot older than I am. I am 36 for your info. Unfortunately it had to get to a point where I can only walk for short distances before I was referred to a Cardio Vascular specialist, and even this was carried out privately, thanks to my employer paying the costs. I am 5’10” and 80kg and never really had a bad diet although I now eat very well, i.e. lots of fruit and veg, nuts, beans, white meat, oily fish and little to no refined sugars or carbs. Up until the point where my leg held me back, I exercised 3 times a week for an hour doing intense circuit training type workouts which due to the short bursts of exercise, suited my quick fatiguing legs. Funny enough it was at the gym when my leg went from bad to worse in an instance. Anyway, Surprisingly my cholesterol was recently tested and came back at 6.3, up from 5.8 about 2 years ago. Apparently my HDL levels are good but my LDL levels a not good and as a result my ratio of the 2 are not good. I was called into the GP today to review my cholesterol levels. When I explained my current diet my GP said ‘well the only option is statins’. (I would like to clarify I knew very little about statins at this point other than when you start taking them you generally have to keep taking them). I explained that I didn’t like the thought of going onto medication that I would need to keep taking indefinitely and requested that we try changing my diet, so he printed out a leaflet and told me to go for a blood test in 3 months time (the leaflet advises using Flora margarine and consuming low fat options of foods of which according to Tim Spector, the author of the diet myth, are the complete opposite to what I should be doing unless I want to poison my body with synthetic spreads and put on weight with sugars). I since read some of the info on your website and am pleased I pushed back. I am however left with many questions. Mainly, do you think my cholesterol levels have anything to do with my PAD? If it materialises that I have FH, how does this get diagnosed for sure and what are the options other than statins. I have an appointment with my doctor the beginning of next month to discuss my options in regards to treatment of my blocked arteries and I have a feeling he is going to focus on my cholesterol level and strongly suggest that I take statins so I want to be fully informed at that point. FYI, I used to smoke from around 16 to 27 years old although I haven’t smoked since then, apart from the odd one on a night out (the specialist has claimed it is this that is the reason for my PAD). Any advice would be good.
thanks
Jim
Hi Jim
I’m sorry but I can’t give advice – I’m a PhD, not MD – not that an MD would give you advice over a blog either! I can share info. Other people you may value are http://www.thefatemperor.com/
and https://drmalcolmkendrick.org/
For your young age, your PAD is understandably worrying for you. However I (and others who think that the assumption that cholesterol is the culprit has caused way more harm than good) would suspect that there is a hereditary/genetic factor here. The smoking won’t have helped, but there is evidence that stopping for a few years can return someone closer to never smoked results, so I wouldn’t blame the smoking for everything. In my opinion, statins would make things worse – you’d be even less able to move and more in pain. This post links to many others (https://www.zoeharcombe.com/2015/03/worried-about-cholesterol-andor-statins/) – check out how statins ‘work’ especially – as well as the ‘normal’ post, because your cholesterol is not high.
I would check HbA1c if I were you – at a recent conference I saw evidence for the association between heart disease and diabetes – so strong that you barely see some risk factor levels in patients that DON’T have diabetes. Sugar is a far more alien substance to the body than natural dietary fat (FLORA should be consigned to the bin in my view!)
You don’t have FH – 1 in 500 do and they invariably have cholesterol in the double figs even on statins. You could get the genetic test, but I think it would be a waste of time. Your chol is below normal – they just move normal!
Good luck with everything – you do need to get to the bottom of the PAD, cos the cause isn’t cholesterol – the cholesterol is trying to fix you!
Best wishes – Zoe
Hi Zoe
Thanks for you comments and links, they are very helpful indeed.
I can’t believe just how twisted this whole cholesterol thing is! I was curious as to who sets the chol levels and why; I found that apparently the ‘National Institute for Health and Care Excellence’ sets the levels but, via a brief Google search, I couldn’t find anything to confirm the explanations for the levels set. There is so much contradictory info out there, it is clear why people can end up confused, me included.
I have looked further into my PAD as you suggested and found information on a potential cause called Endothelial Dysfunction, which is basically a thin layer on the inside of our arteries, veins and vessels that aids the flow of blood. Apparently if the layer is damaged it could be vulnerable to cholesterol penetrating and sticking and leading to Atherosclerosis, thus resulting in PAD. I read one article (http://circ.ahajournals.org/content/115/10/1285) that suggests Atherosclerosis starts in childhood which is interesting. Anyway I will keep searching and see what other possible causes I can find before my consultation next week.
Thanks again
Jim
You write, “I now eat very well, i.e. lots of fruit and veg, nuts, beans, white meat, oily fish”. I disagree that “fruit and veg, nuts, beans” are as good as you think due to their anti-nutrients, & I think your preference for “white meat” displays a bias against saturated fat & robs you of the nutrients in red meat. Eggs are also a great source of nutrition.
Hi I recently had a lipid panel done and everything has changed, gone up, the Dr is thinking about putting me on Statins but i am going to refuse. My mother, sister have high cholesterol. I was diagnosed with CLL last April and have had Dr. appts here , there and everywhere, biopsies etc. The last 6 months have been very stressful for me. Prior to that i was pretty much stress free and living the good life. My question is do you think stress can play a role in high cholesterol ? I have also been on a raw veggie diet the last 6 months , could that also effect the counts? Thank you
Hi Peggy
I’m really sorry to hear of all the things you’ve been going through and the stress this has understandably put you under.
You may find my main post on cholesterol and statins interesting (https://www.zoeharcombe.com/2015/03/worried-about-cholesterol-andor-statins/)
The short answer to your question – can stress play a role in (high) cholesterol? Absolutely. Even the stress of the appointment affects the results – one of the links from that main post shares the inaccuracy of the test (19% for starters!)
I’m personally not sure about a raw veggie diet – especially when fighting serious illness. A number of nutrients are only found in foods of animal origin and meat/fish/eggs/dairy are nutrient dense (https://www.zoeharcombe.com/2014/04/healthy-whole-grains-really/) Cutting out junk is a great idea, but not cutting out highly nutritious foods.
All the best for your appointments
Best wishes – Zoe
HI Zoe,
I am 42 have been diagnosed with high cholesterol at total 7.2 on average for the last 2 years. I had a test for FH which came back negative. Just recently I had another test and it shot up to total 8.6, but LDL 6.2, TRI 1.4 and HDL 1.7. I am tall and not overweight.
I discussed this with my Cardiologist who said that I have FH, I told him about the test I had that was negative, but he seemed convinced that I have it, citing that there is probably another gene I have that has not been discovered yet, and says I should get a CT calcium score done, and probably be on statins or injection statins.
My mum and dad both have high cholesterol and are on statins, but they are both still around thankfully and in their 70s. My dad recently had a bypass at 72 though. I’d be interested to know if you think i should get a second opinion?
Hi Tim
I actually gasped out loud when I read the bit about the gene that’s not been discovered yet. WTF?! How can a so-called professional bare faced make up something like that?!
The injection statins comment make sense. It explains this person’s (I can’t bring myself to call him a doctor) enthusiasm to ensure that you have FH (when you clearly don’t – by having a completely normal chol level and/or by genetic confirmation). At the moment, the wildly lucrative drugs (with largely unknown consequences) are only allowed for those with FH. Check this out: https://www.zoeharcombe.com/2016/04/pcsk9-inhibitors-statins/
You may also find this interesting (https://www.zoeharcombe.com/2015/03/worried-about-cholesterol-andor-statins/) Ideally, you would never have ‘got into the system’ but, given that you have, – check out the link from this post that goes to the post about “normal”. You are as normal as chol is (when they don’t statinate).
Read the leaflet in your parents’ statin meds and read the bit about caution being advised for over 70s being in statins (because chol is even more important for older people – it’s pretty flipping vital for younger people too). Then maybe go and ask your parents’ doc(s) if they have read the leaflet and if so WTF are they doing?!
If your higher score (still not that high) was recently and you live in the N hemisphere, this will be a reflection of lack of sunshine. Sunbathe sensibly as soon as the nice weather returns and then the body makes vit D from cholesterol – that’s one of the many, many reasons why the body makes cholesterol.
I’m still in shock at your doc – he should be on a TV prog about con men!
Best wishes – Zoe
Thanks for the reply Zoe . I read with interest all of your articles about this and to me it makes perfect sense . I am still a bit confused though . Do you know also if having kidney stone and also gum disease is linked to high cholesterol and or Athercolosis ?
I am now not sure whether to go for the scan or not ? Confused .
Hi again – yes good one – I was so shocked I missed the CT test query!
My go to person for proper heart disease doc views is this chap (https://drmalcolmkendrick.org/2016/03/22/what-causes-heart-disease-part-x/)
You’ll enjoy reading his other posts too – this is part X of a series that’s over XX by now – you will probably enjoy them all.
I would worry more about the guy who makes up genes going anywhere near me again than I’d worry about the CT scan! It looks like it can tell you some interesting things, but it’s by no means definitive. I simply wouldn’t trust gene-make-up-man to be unbiased when sharing the results. I get the impression he wants to try another test to get you on PCSK9s. Do ask him if he is being paid to find patients for this new drug!
Best wishes – Zoe
p.s check out this guy’s posts too – he’s worked out how to use fat to drop cholesterol and explains how! http://cholesterolcode.com/how-to-do-the-cholesterol-drop/
Given that I don’t care about cholesterol, I wouldn’t play any games with it – but this – or sunbathing – could drop cholesterol if you were bothered!
Hi Zoe, so much seems familiar in these comments regarding my questions, lack of answers from medicos and questions of how did I get to this condition?
I’m 59 recently had a heart attack, cardiovascular disease, stent put in and usual recommended treatments of drugs; including statins.
I had a bad reaction to statin treatment and gave them the flick pretty quickly, much to the disdain of my consultant doc.
Short version question is… How did I get this plaque build up in my arteries and can I reverse it?
Yes I have been a smoker, but also a very active person my whole working life with a pretty non diet based eating regime i.e I have been a very fit and active person for a long time and gave up smoking for over 10 years, then bang, complete blockage of left descending thing in / on my heart. Lucky to be here I guess.
Any comments on how it all got to this and the other drugs I’m on like brilinta, metoprolol,ramipril and aspirin.
Feeling like a guinea pig
regards
Sean
Dr Harcombe,
Could you please point me in the right direction to study up on high blood pressure (HBP) probably due to high T3 hormone. I need the latter because I had thyroid cancer so I have no thyroid. I am terrified to go to the doctors (with my HBP) because I think he will put me on some god awful blood pressure lowering drug which will cause more problems than I have at the moment. I am also stuck because I know that thyroid medication interferes with blood pressure lowering drugs (they both use the availableTBGs).
Where do I start Dr H? It took 3 years to get my thyroid meds to an optimal level and ratio, I don’t want to have to do all that again.
Hi Lahs
My first thought would be – do you genuinely have high BP? This may help https://www.zoeharcombe.com/2014/06/diabetes-cholesterol-bp-normal-is-no-longer-normal/
The true average is about 140/90 and anything on the normal distribution is normal – by definition!
There’s nothing that jumps out with a quick pub med search (academic articles). This looks interesting and has some good academic refs http://www.medscape.com/viewarticle/733788_1
I really would be challenging what is considered normal for BP
You’ll enjoy this just for support/interest https://drmalcolmkendrick.org/2015/05/01/treating-thyroid-patients-like-children/
One of the best ways of lowering BP quickly if you’re interested is a low carb diet. Any carbs that are not used up by the body (and most people with access to food eat more carbs than they need most days) are stored as glycogen (and then turned to fat) but we can keep a steady glycogen level of about 500g in the body at any one time. For every gram of glycogen, the body holds 4 grams of water. Think of a pressure cooker – more water = more pressure. The body is similar. If you keep your glycogen levels low (anything below 150g of carb a day should help) – your water held is also lower. If you do a very low carb day (nearer 50g of water) you can lose 5lb ‘overnight’ and BP drops noticeably.
Hope this is of interest
Best wishes – Zoe
Hi Zoe.
Thanks so much for putting my mind at rest. Perfect timing. Got my FH results today. Negative.
Although they say it’s likely I’ve polygenic Hypercholesterolemia.
My TC after intermittent fasting were 15.9 and 15.8, LDL 12,6, HDL 2.7 Trigs 1.
This weeks fasted bloods after a meal of chicken and peppers baked in Philadelphia cheese topped with Parmesan were TC 12.6 LDL 8.9 HDL 2.8 and trigs 0.8
Then consultant said the only time he had seen such high results were in an anorexic. Makes sense. With a bit of tweaking in my diet I’m sure I’ll get there.
Kind regards
Annette
Hi Annette – well I’ve never heard of polygenic Hypercholesterolemia before and I suspect it’s a conveniently made up term!
“This condition is caused by a susceptible genotype aggravated by one or more factors, including atherogenic diet (excessive intake of saturated fat, trans fat, and, to a lesser extent, cholesterol), obesity, and sedentary lifestyle. The involved genes have yet to be discovered.” (http://emedicine.medscape.com/article/121424-overview) I bet they have ho ho!
This may be of interest (https://www.zoeharcombe.com/2015/03/worried-about-cholesterol-andor-statins/) Especially the link to the Fraser paper showing a 19% difference in chol test readings is pretty much to be expected! (http://www.bmj.com/content/298/6689/1659) The whole thing is a joke
Best wishes – Zoe
Hi Dr Harcomb,
This may not be the best way to enter this discussion, but thought you might be interested in my story. I’m 70, have HeFH with LDL alone over 500 mg/dl, yet by Electron Beam Computed Tomography, done 5 times over a decade, my coronary calcium burden is zero. My last stress ultrasound showed my heart to be decades younger than my chronological age. After much searching I finally found a Harvard researcher that seems interested in me (and my similar older sister, who also has HeFH and a low calcium score). I donated a blood sample, but have found out I will probably never hear any results of any investigations. What I find perplexing is the persistent belief that I “must have something that is protective” from the “obviously dangerous effects of elevated lipids”, rather than my idea that I simply don’t have the “something else that causes plaque”. Occam’s razor says to me that a single explanation (absence of plaque forming gene?) is much simpler than a two part explanation (presence of plaque forming gene PLUS presence of plaque protective gene). Only when the single step explanation must be excluded should anyone consider the two step solution.
Hi Rwbramel
Thanks so much for sharing this – quite fascinating!
I think that’s most unfair that you give bloods and they don’t give the results back! I would make any future help conditional on a return.
Have you come across this blog? https://drmalcolmkendrick.org/ If you look at the (now over 20) parts of the What really causes heart disease post, you may find many ‘black swans’ that don’t add up and hypotheses that do. Cholesterol per se is protective – it’s just most people are too wrapped up in the diet heart hypothesis to realise this!
Hopefully my blog was of interest in that, having made it this far, you (and sister) are highly likely to be around for many more years to follow! And with a sharp mind by the looks of it :-)
Best wishes – Zoe
Hi,
My husband (62) has recently suffered a couple of attacks of angina. He will be getting a chest x-ray soon just to check it’s not a lung problem.
He has a cholesterol reading of 8 which is high, this seems paradoxical given that he is not overweight at all, keeps himself very fit, doesn’t smoke, eats a healthy diet with plenty of vegetables etc. I switched him to butter about 5 years ago as up until he and I got together his ex had been buying the flora type stuff and also Elmlea instead of cream! He hardly eats any dairy apart from cheese. He doesn’t eat desserts and I also got him to stop putting sugar in tea (he still has it in coffee) and to cut down massively on biscuits (now one a day).
It’s such a shock for us to find someone as fit as he is suddenly finding it a struggle to complete 7 lengths of the pool non-stop when he had previously been quite easily managing 50. When I say he is fit he has a BMI of 23, he is on his rowing machine for 30 minutes a day. He has never smoked and drinks very moderately – i.e. nurses half a pint in the time it takes the rest of the group down a couple of pints.
His father had a heart attack at 49 so we are wondering if it is FH.
I know you cannot possibly give a diagnosis or any medical advice in this setting. But I would be interested in hearing your thoughts on what investigations we ought to seek.
Hi Frances
I’d be astonished if a reading of 8 were indicative of FH. There can be other hereditary heart conditions not connected to FH (indeed, given the rarity of FH, other factors are more likely).
It seems like you’re doing the right thing getting this checked out urgently (I hope your appointment is v soon?) Angina can be confused with heartburn but anything that seems like chest pain requires immediate attention. The “struggling to swim 7 lengths when 50 previously was easy” is worrying. There may be circulatory issue with such breathlessness. There could also be other reasons for this e.g. panic attacks/extreme anxiety for some reason – but this all needs urgent medical examination.
I can’t advise but I would suggest getting to a doc pronto!
Best wishes – Zoe
Thank you very much for your reply Zoe. It is very worrying. I am concerned it may be something to do with living in a house that is only heated by wood burning stoves and old ones at that. He has been put on the waiting list for an angiogram but there is a wait of 24 weeks!
Thanks again for the reply.
Hi again – I thought about something more reassuring – hopefully father had other risk factors that hubby doesn’t? smoking? sedentary lifestyle? risky job? exposure to something? We don’t inherit everything!
Good luck with everything
Best wishes – Zoe
Hi Zoe, I have FH which my mum, brother and I all have. We think my mothers father may have had it, as had heart disease and died of a heart attack. My gp referred me to an endocrinologist at the hospital. They tried me on every statin going and I had terrible side effects and the main one being muscle problems that made me feel like an old man.
So, I couldn’t tolerate any statin on the market. They then tried me on Ezetimibe with again, terrible side effects which I couldn’t tolerate. They ended up putting me on Omacor ( an oil capsule). I take two a day and this keeps my tryglicerides at a lower level. Unfortunately, the medical profession at times have not updated themselves with the latest research and they even at one point told me not to eat eggs !!!!
Do you know if the Omacor is sufficient for me, or should I be taking anything else to take to stimulate the cholesterol and if so, where would I get this from, as I know for certain my gp won’t give me this.
(I’m loving the diet and have lost 12 pounds of weight in the first two weeks and really enjoying and sticking to phase 2).
Hi Michael – huge congrats on your weight loss and good to hear you’re enjoying how you’re eating :-)
I can’t advise on any personal health issue – I’m sorry to hear you’ve had such bad experiences with attempts to lower cholesterol (but not surprised) – this FH article may offer an explanation. If you genuinely have FH (genetic defect confirmed, not presumed), your cells will already be suffering from low LDL – statins would make this worse.
This article explores statins and cholesterol more widely and may be of interest https://www.zoeharcombe.com/2015/03/worried-about-cholesterol-andor-statins/
Avoiding carbs lowers triglycerides interestingly enough – so more fat meals and fewer carb meals in Phase 2 and your triglycerides may go lower still.
I don’t think there is anything that stimulates cholesterol production and, you’re right, it would unlikely ever be prescribed! My personal view is just leave the body’s brilliant, incredible cholesterol mechanism alone and it will do what it can do. With genuine FH people, it is impaired, but the body’s ability to adapt is also incredible.
Let’s hope your body is adapting as well as your mind!
Best wishes – Zoe
Hi Zoe, I just wanted to say a big, big thank you to you and your husband. I have been on the diet for three weeks and have lost 19 pounds in weight. The main thing is that I discovered that I had a serious problem with yeast and candida and had really bad candida die-off in the first two weeks. I kept on phase 2 and then had some wholemeal bread without sugar, made in our bread machine.
The day after my symptoms returned and it also has when I have had a glass of wine. It appears to be a yeast intolerance, linked to candida. I realise now that I had been suffering for years with leaky gut, chronic fatigue and related inflammatory health problems. I have also suffered with anxiety all my life and the information I have read, links anxiety and depression (again which I have had a few times) to candida and yeast intolerance.
The good news is that I have so much more energy, feel good, am sleeping for 7 hours a night compared to 12 and 13 hours I sometimes used to sleep. So, thank you once again and this is an eating plan for life for me now and it has turned my life around completely. :)
Hi Michael
Thanks so much for letting us know! It’s so lovely to get an update like this. We’re so pleased that this has helped you.
It’s a bit tough when there are things that are no longer able to be tolerated, but best to know and then decisions can be made. Andy is fine with wine but tends to suffer quickly and badly with beer, so he has a choice. He’s at the match (Wales SA) next weekend, so he may well have a beer – but he knows what will happen so he also might not!
Great to hear about the energy and sleep too – keep up the fab work!
Best wishes – Zoe & Andy
Hi Zoe,
I just want to say thank you for these very interesting posts.
My mom showed me an article in the Telegraph about paper you linked above about giving statins to babies and I think i screamed out loud! – especially now as a new Dad.
Unfortunately I believe it will take a generation to change people’s mindset about cholesterol especially when you have to declare having ‘high cholesterol’ when getting life insurance!!
Tom.
Hi Zoe–
Per our twitter exchanges (I’m @DaveKeto), my N=1 research to date includes 32 NMRs where I identify a very distinctive *inverse* relationship between dietary fat and corresponding LDL cholesterol (-C, -P, and Small -P). I further recruited my sister (who has a very different lipid profile) for the Identical Diet experiment where we ate exactly the same food (including weight) for 13 days and took 7 NMRs which likewise show matching inversions and tight pattern correlations with each other’s numbers (http://cholesterolcode.com/cholesterol-code-part-v-more-fat-less-cholesterol-to-the-second-power/).
In the most recent experiment I induced a record drop in my cholesterol over 3 days in the first public presentation of my data with LDL-C dropping by 73 and LDL-P dropping by 1115! (http://cholesterolcode.com/cholesterol-code-part-v-more-fat-less-cholesterol-to-the-second-power/)
I bring this to your attention with regard to FH in particular. The lipid system is FAR more agile and responsive than modern medicine believes it to be. My own data is putting to rest the clearance presumption as showing much stronger evidence that the body is in fact up and down regulating lipids based on incoming energy (and mostly likely dietary fat). This is particularly relevant to FH as it is a foundation for the argument that high cholesterol is atherogenic.
Their theory: FH mutated LDLr => lower binding to LDLp Apos => higher cholesterol remaining in the blood — Low “clearance” leading to metabolic “backing up” of serum cholesterol.
But what everyone seems to be missing is that there’s a particularly GOOD reason for a system with FH to ***upregulate*** LDLp.
If you, Zoe (who doesn’t buy into the diet-heart hypothesis like so many of us) knew you had FH and thus your cells had poor reception to LDL particles that your cells desperately need for energy, nutrition, and repair — you’d want to *stimulate* LDLp production! Why have 500 LDLp when you could have 1000? 2000? Whatever it took to ensure proper saturation of these vital elements needed throughout your body. Give those poor LDLrs more opportunities to bind by providing more targets.
Remember bobbing for apples? If those apples were the only way your kid would eat and having a few in the barrel was just too hard for her compared to others, you’d go ahead and fill the bucket until it was easy.
People dying more often of CVD with FH doesn’t surprise me given the LDLr is a critical pathway to proper cell nourishment and thus I’d assume there’s more endothelial damage/dysfunction under such circumstances. But for goodness sake, if this does turn out to be true, adding a statin is one of the very last things I’d ever do.
Hi Dave – lovely to e-meet you! Looks like we came to the same conclusion – FH needs something to stimulate LDL production!
I’m following you now – keep experimenting! This is one to bear in mind – the complete inaccuracy of the whole shooting match anyway http://www.bmj.com/content/298/6689/1659
Best wishes – Zoe
I recently had my LDLp counted: 3,500. It was highlighted as too high. Should I be worried or is it a good thing after all?
LDL particle size: large buoyant only, no small dense.
Total cholesterol: 11.25
HDL is fine, triglycerides low, LDL 8.25
I was told in 1991 that I had FH. I was 24 and put on statins, which I took for 8 years, then decided to stop. Every since then, I have had to defend my decision to doctors. A gene test has now revealed that I do not have FH.
Dave,
Your work is truly groundbreaking! I enjoy using it, along with Zoe’s, in disrupting the conventional wisdom of medicine. So what could the FH patient do to improve endothelial function?
Keep up the impressive work!
Roger
Dave and Zoe, you are both amazing! I’m so thankful to have found the information you both provide. I’m 33 years old and was diagnosed as having FH at age 22 based on LDL (as well as lipoprotein a and ApoB) after my father died of a heart attack at age 56. My sister’s lipid markers were all very similar to mine and we were both prescribed statins. I reluctantly started them even though I knew there was barely any good evidence on this topic (I was a pharmacy student at the time). I had to stop the statin when it was time to start a family and the cardiologist told me “you better have your kids as close in age in possible and get right back on your statin”. I was terrified! Fast forward to today, we have 1 child but want another one and so I have not gone back on the statin. After all my research over the past few years and becoming enlightened on the cholesterol controversies, I don’t think that I will ever go back on one. But my first step before deciding anything is to get a genetic test to confirm the FH diagnosis (imagine I’ve been living in fear for 10 years over something that is not true!). I can’t believe people are diagnosed without this and so far getting the test has proven difficult (I’m seeking out ways to access it and pay for it privately). Being told you have FH and “will die young with no statin” is so terrifying. I was also told that there was nothing I could do to lower my lipoprotein a which put me in the “very high risk” category. Well after 1 month of a low-carb diet, my level now puts me in the “low risk” category. I was shocked. And all of my other lipid markers are the best they’ve ever been (besides LDL and ApoB which are slightly higher). There are definitely moments where I question what I am doing and get nervous that I am not on a statin while my sister is. But at the same time, I feel like my hands are tied anyway since we want to have another child. Bottom line is that the evidence for statin use, even in FH patients, is not nearly compelling enough for me to think it would do anything more for me than having all of my other risk factors minimized already. Anyway, I just wanted to thank you for giving me (and all other “possible” FH patients living in fear!) some sanity and peace of mind in all of this madness.
Forgot to mention that my most recent LDL level was 5.38 mmol/L
Hi Lisa
Thanks so much for sharing this – you’ve got a 1 in 500 chance of having FH so the test result will be interesting!
Best wishes – Zoe
Hello.
I have two earlobe creases and high cholesterol 8.1 although my lipid test didn’t show any genetic cause of concern. Should I be concerned about earlobe creases?
Zoe,
Starting the programme today with a great deal of optimism that four years of health problems’ symptoms’ treatment may come to an end by treating diet as the root cause. We’ll see what happens – I am optimistic because it all makes sense.
One thought about the 3,500 in = 3,500 out debate: it may actually not be as wrong as you believe. Let me explain my thinking. We now know a lot more about the microbiome and are beginning to realise that what goes into the mouth does not necessarily enter the body (as well as learning that what sometimes enters the body through the gut really shouldn’t – my problem I think is inflammation). So 3500 calories into the body may well need to equal 3500 calories out to lose weight but 3500 calories in the mouth doesn’t necessarily equal 3500 into the body.
If my thinking is not too far from the mark, it will equal a seriously wide variance depending on individual microbiota make-up. Far from an expert in this so very interested in your thoughts.
Hi Kev
I guess you’ve seen this post? https://www.zoeharcombe.com/2014/06/the-calorie-theory-prove-it-or-lose-it/
This one may also help explain why calories – especially 3500 – are just not helpful http://www.theobesityepidemic.org/2014/02/a-calorie-is-not-a-calorie-and-heres-the-reason-why/
Good luck & best wishes – Zoe