
Replacing, not lowering, cholesterol would be more accurate
You Magazine, Mail on Sunday (18 & 25/5/14), featured a new book by Ian Marber and Dr Laura Corr, with recipes by Dr Sarah Schenker, called “Eat your way to lower cholesterol: Recipes to reduce cholesterol by up to 20% in under 3 months”.
My first thought, upon seeing the title, was – why would anyone want to lower cholesterol? Sadly, this will be the last thought of most people browsing amazon or a book shop. Everyone nowadays wants to lower their cholesterol – that’s how successful the cholesterol lowering industry has been at demonising this life vital substance in the name of money.
Lowering cholesterol – General consensus vs. evidence
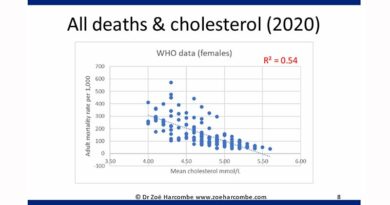
Stop 100 people in Queen Street, Cardiff, and 99 will tell you that cholesterol is bad and the lower one’s cholesterol level the better. Now may be a useful time to remind people of the true relationship between cholesterol and deaths. Scroll down the blog post until you see four graphs showing the following:
– The higher the cholesterol, the lower the deaths from CVD (cardiovascular disease) for men;
– The higher the cholesterol, the lower the deaths from CVD (cardiovascular disease) for women;
– The higher the cholesterol, the lower the deaths from any cause for men;
– The higher the cholesterol, the lower the deaths from any cause for women.
This is pure (not-played-with) data from the World Health Organisation for 192 countries. That’s just about as good as data gets and it shows the exact opposite of what we’re being told.
This is raw data – what about studies?
The Honolulu Study (Ref 1) was a 20 year study of cholesterol levels and mortality in 3,572 Japanese American men. The study concluded that “Only the group with low cholesterol concentration at both examinations had a significant association with mortality”. The authors added “We have been unable to explain our results”. (I.e. we were expecting lower cholesterol to equal lower mortality, not the other way round).
Framingham (the longest and probably best known population study ever) similarly concluded: “There is a direct association between falling cholesterollevels over the first 14 years and mortality over the following18 years (11% overall and 14% CVD death rate increase per 1mg/dL per year drop in cholesterol levels).” (Ref 2) Dr Malcolm Kendrick did a clever calculation on this finding and translated this into – a reduction in cholesterol from 5 to 4 mmol/L would increase your risk of dying by 400%.
Elaine Meilahn reported in Circulation (2005) “In 1990, an NIH (National Institutes of Health) conference concluded from a meta-analysis of 19 studies that men and, to a lesser extent, women with a total serum cholesterol level below 4.2 mmol/L exhibited about a 10% to 20% excess total mortality compared with those with a cholesterol level between 4.2 and 5.2 mmol/L.” (Ref 3)
Still want a book claiming to lower your cholesterol?
Lowering cholesterol through diet – how?
The 18/5/2014 You Magazine article has a box-out called “six superfoods” to boost heart health“. Notice how lowering cholesterol has already become interchangeable with heart health? Before you reach the end of this article you will see that there is no evidence whatsoever for that claim… quite the opposite in fact.
The six superfoods are claimed to be fibre; healthy oils (described as those high in unsaturated fat of course); soya; nuts; oats and ‘smart foods’. Smart foods are defined as margarine-like spreads and other fortified foods that claim to “actively lower you cholesterol” (those yoghurt/drink/one-a-day kind of things).
The only two of these six that I would describe as foods are nuts and oats. Fibre is a component part of carbohydrate (not all carbohydrates contain fibre, but no pure fat/protein contains fibre). ‘Smart foods’ are a category of processed gunge. Oils are nutritionally pointless and they’re a cooking ingredient/dressing, not a food. Soya is a whole different ballgame – see “The Whole Soy Story” by Dr Kaayla Daniel for the Whole Sorry Story on this one.
Which reminds me – please tell me that this book comes with the most obvious possible warning for any female wanting to conceive? Soya alone is a plant oestrogen – think ‘the pill’. It takes a lot of cholesterol to make a healthy baby and lowering cholesterol is the last thing that a would-be-mum wants to do. I’m not sure of the impact on male sperm either – almost certainly not good.
Replacing cholesterol more like
The key thing that this strange list of foods and non-foods have in common is (phyto)sterols. Sterols are added to margarines and other substances that have cholesterol lowering claims. You don’t need to consume these fake and expensive products. If you’re daft enough to want to lower your cholesterol you can buy sterol tablets from a health food shop and save yourself the harm and expense of ingesting spreads or ‘shots’.
Phytosterols are cholesterol-like molecules found in all plant foods, with the highest concentrations found in vegetable oils. They are absorbed only in trace amounts, but they inhibit the absorption of intestinal cholesterol (Ref 4) – human cholesterol in effect. We have known this for 60 years. The ability of phytosterols to inhibit the absorption of cholesterol was first shown in 1953 (Ref 5). (Fibre per se has a similar effect – it reduces the body’s absorption of cholesterol.)
Foods with phytosterols are competing with the cholesterol made by the human body and replacing it to an extent. Not entirely, or we’d drop dead. Blood cholesterol levels will fall, but how is this a good thing? Our bodies make cholesterol. I don’t know about you but I trust mine to make the cholesterol that it needs (so long as I don’t abuse it with statins). If my body needed plant cholesterol – surely it would make plant cholesterol? Do you know the true health impact of replacing your own cholesterol with plant cholesterol? Nope – me neither. And nor does Unilever I suspect.
The European Food Safety Authority responded to a request from Unilever PLC to be able to make cholesterol lowering claims on their plant sterol fortified products (Ref 6). The review body concluded that “plant sterols have been shown to lower/reduce blood cholesterol“. They also stated “However, there are no human intervention studies demonstrating that plant sterols reduce the risk of coronary heart disease.”
You may like to read that again (and You Magazine may like to retract their “boost heart health” claim). Plant sterols lower cholesterol (tick) but there is no evidence that plant sterols reduce the risk of heart disease. Can this mean that lowering cholesterol per se does not reduce the risk of heart disease? It sure does. However, there’s an even more important question to ask.
Is this even safe?
The area of most interest to us is phytosterol consumption and cardiovascular disease – as this is the area where health claims are made. There are a few studies of phytosterol intake and cardiovascular disease:
Rajaratnam et al studied the association of phytosterols and coronary artery disease (CAD) in postmenopausal women (Ref 7). They concluded that women with elevated ratios of sterols to cholesterol [i.e. plant cholesterol to human cholesterol] have enhanced risk for CAD. “Thus, enhanced absorption and reduced synthesis of cholesterol may be related to coronary atherosclerosis.” (My emphasis on enhanced risk).
Sudhop et al reviewed plant sterols as a potential risk factor for coronary heart disease (CHD) (Ref 8) and confirmed a strong influence of plant sterols. They concluded: “These findings support the hypothesis that plant sterols might be an additional risk factor for CHD.” (My emphasis on risk factor).
Assmann et al’s 2006 article concluded: “Elevations in sitosterol concentrations [one type of sterol] and the sitosterol/cholesterol ratio appear to be associated with an increased occurrence of major coronary events in men at high global risk of coronary heart disease.” (Ref 9) (My emphasis on increased occurrence of major coronary events).
Silbernagel et al studied 1,257 individuals in the Ludwigshafen Risk and Cardiovascular health (LURIC) study (Ref 10). They found that high absorption of phytosterols alongside low synthesis of cholesterol predicted increased all-cause and cardiovascular mortality in LURIC participants. (Naughty me again emphasising the finding that sterols replacing human cholesterol predicted dying.)
Summary
It has become so well known that ‘lowering cholesterol is a good thing’ that we are forgetting to challenge the entire and immense industry that has followed from this (drugs and spreads). Lowering cholesterol is a bad thing and replacing cholesterol with plant sterols is a very bad thing. These bad things are made even worse if the human being tampered with is of child bearing age/has parent-like aspirations. It’s also very bad for any human who wants to live longer. But, what the heck, so long as the cholesterol lowering industry is worth billions – who cares?!
References:
1) Schatz, Masaki, Yano, Chen, Rodriguez and Curb, “Cholesterol and all-cause mortality in elderly people from the Honolulu heart programme”, The Lancet, (August 2001).
2) Anderson, Castelli and Levy, “Cholesterol and Mortality: 30 years of follow-up from the Framingham Study”, Journal of the American Medical Association (JAMA), (1987).
3) Elaine Meilahn, “Low serum cholesterol: Hazardous to health?” Circulation, (2005).
4) Ostlund, R. E., Jr. (2002) Phytosterols in human nutrition. Annu Rev Nutr. Vol.22 pp.533-49.
5) Pollak, O. J. (1953) Reduction of Blood Cholesterol in Man. Circulation. Vol.7(5), pp.702-706.
6) Bresson, J.-L. (2008) Scientific Opinion of the Panel on Dietetic Products Nutrition and Allergies on a request from Unilever PLC/NV on Plant Sterols and lower/reduced blood cholesterol, reduced the risk of (coronary) heart disease. The EFSA Journal. Vol.781 pp.1-12.
7) Rajaratnam, R. A., Gylling, H., and Miettinen, T. A. (2000) Independent association of serum squalene and noncholesterol sterols with coronary artery disease in postmenopausal women. J Am Coll Cardiol. Vol.35(5), pp.1185-91.
8) Sudhop, T., Gottwald, B. M., and von Bergmann, K. (2002) Serum plant sterols as a potential risk factor for coronary heart disease. Metabolism. Vol.51(12), pp.1519-21.
9) Assmann, G., Cullen, P., Erbey, J., Ramey, D. R., Kannenberg, F., and Schulte, H. (2006) Plasma sitosterol elevations are associated with an increased incidence of coronary events in men: results of a nested case-control analysis of the Prospective Cardiovascular Munster (PROCAM) study. Nutr Metab Cardiovasc Dis. Vol.16(1), pp.13-21.
10) Silbernagel, G., Fauler, G., Hoffmann, M. M., Lutjohann, D., Winkelmann, B. R., Boehm, B. O., and Marz, W. (2010) The associations of cholesterol metabolism and plasma plant sterols with all-cause and cardiovascular mortality. J Lipid Res. Vol.51(8), pp.2384-93.


Hi Zoe,
Please could I have your opinion?
I have recently had bloods tested and was advised I need to start statins. Having already read ‘The Great Cholesterol Myth’ and following your website I have refused.
My overall Cholesterol was 7.9 (supposedly sky high)
My HDL were within the normal range
My Triglycerides were within the normal range
However my LDL was 6.07 which is high giving me a ratio of 5.8
I am aged 40 in good health and weigh 162 Lbs. I do have hypothyroidism but have no history of heart problems.
Despite everything I have read about the dangers of statins, I am still unsure as I have not found any data on anyone that has the same values as me.
Many thanks,
SteveC
Hi Steve
I recently posted this blog to answer cholesterol queries. I think you can stop at point 1 – is 7.9 high? Er – no!
https://www.zoeharcombe.com/2015/03/worried-about-cholesterol-andor-statins/
Best wishes – Zoe
p.s. I highly recommend Dr Malcolm Kendrick’s The Great Cholesterol Con on all the HDL/LDL/ratio nonsense. It goes something like this…
Cholesterol causes heart disease.
No it doesn’t.
Well LDL causes heart disease …
No it doesn’t.
…and HDL prevents it.
No it doesn’t.
So it’s the ratio of HDL to LDL.
No it isn’t.
So there are big fluffy LDLs and small dense ones.
Oh when will you just shut up and admit you were wrong!?
Hi Zoe – thanks for all the fascinating info. I’m trying to convince a friend on statins that he should take no notice of his so-called ‘too high’ cholesterol level, and leave the statins. Am I right in thinking that measuring a broad cholesterol level is at any rate of no use? To know anything about his cardio-vascular health, should his doctor rather be telling him his triglyceride level, HDL level, and LDL level? And if yes, what would the ‘correct’/healthiest levels be??? Thanks so much, regards Andrea
Hi Andrea
In my view, the cholesterol test is worse than useless – because it all too often results in people taking drugs that can do harm and not good – and the component parts are equally pointless. They are just all part of the moving goal posts as the cholesterol myth catches up with its believers..,
First they say it’s total cholesterol. When this doesn’t correlate (https://www.zoeharcombe.com/2010/11/cholesterol-heart-disease-there-is-a-relationship-but-its-not-what-you-think/), they say it’s good and bad cholesterol. There is no such thing. Cholesterol is cholesterol. C27H46O is the formula – there is no good or bad version. HDL and LDL are lipoproteins, not cholesterol. They’ve even tried claiming it’s the ratio of HDL to LDL or differences in particle size – as Dr Malcolm Kendrick says – when will you shut up and just admit you were wrong?!
Your friend may like to know:
1) The total cholesterol test is inaccurate for starters (http://www.bmj.com/content/298/6689/1659).
2) The component parts are guessed, not measured. The formula blood cholesterol levels is: Total cholesterol = LDL + HDL + triglycerides/5 (https://www.zoeharcombe.com/2012/08/cholesterol-what-does-the-blood-cholesterol-test-actually-measure/)
Few people know that we can only measure total cholesterol and HDL with the standard blood test. Yes – 1 equation, 4 unknowns, 2 measurable = not very scientific.
3) What statins actually do in a human (https://www.zoeharcombe.com/2013/10/how-statin-drugs-really-lower-cholesterol-and-kill-you-one-cell-at-a-time/)
4) Even if your friend has already had a heart attack, he has a 98.2/100 chance of statins doing nothing for him anyway (http://drmalcolmkendrick.org/2014/12/01/what-is-t/)
I would buy him The Great Cholesterol Con by Dr Malcolm Kendrick and that should make his own mind up!
Best wishes – Zoe
Thank you for pointing out this under discussed finding. I checked a bit further on the studies about low cholesterol. In a useful review Low Serum Cholesterol Hazardous to Health? by Elaine N. Meilahn, MD, it is noted that in the Honolulu Heart Study, “Results showed the expected association of elevated cholesterol with coronary disease. ” But there was a rise in non coronary deaths. This latter finding she says “provide(s) evidence that the association previously reported between low cholesterol and noncoronary mortality probably reflected the cholesterol-lowering metabolic consequences of long-term subclinical disease rather than a hazard associated with low cholesterol per se.” She follows this up.
“This conclusion [that something else causes lowered cholesterol and that thing also causes mortality] is consistent with results of a recent meta-analysis10 of cause-specific mortality (including unpublished data on noncardiovascular causes of death) from 10 large cohort studies and 2 international studies that concluded that reduced serum cholesterol is not related to excess mortality among cohorts of employed individuals, whereas population-based studies did show a relationship. The investigators proposed that the discrepancy in results was probably due to a higher frequency of risk factors associated with low cholesterol, eg, alcohol abuse and ill health, in population-based study samples compared with employed cohorts.”
Clearly more research must be done. But it might be nice to note the possibility that in population studies lowering cholesterol may be more an indication that something else is wrong.
Hi DK – I quote Meilahn in a section on cholesterol and mortality in my obesity book along with other findings on cholesterol and mortality (extract below).
There’s a fab book by David Evans called “Low cholesterol leads to an early death” with evidence from 101 papers on this topic.
You may also like this post on the global correlation between (high) cholesterol and (low) mortality https://www.zoeharcombe.com/2010/11/cholesterol-heart-disease-there-is-a-relationship-but-its-not-what-you-think/
Best wishes – Zoe
“The Honolulu Study (ref 1) was a 20 year study of cholesterol levels and mortality in 3,572 Japanese American men. The study concluded that “Only the group with low cholesterol concentration at both examinations had a significant association with mortality”. The authors went on “We have been unable to explain our results”. (I.e. we were expecting lower cholesterol to equal lower mortality, not the other way round). All credit to the team for their honest reporting of these unexpected results and their final statement in the abstract: “These data cast doubt on the scientific justification for lowering cholesterol to very low concentrations (<4•65 mmol/L) in elderly people.”
"Framingham similarly concluded that “There is a direct association between falling cholesterol levels over the first 14 years and mortality over the following 18 years (11% overall and 14% CVD death rate increase per 1 mg/dL per year drop in cholesterol levels).” (Ref 2) Kendrick does a clever calculation on this quotation and translates this into – a reduction in cholesterol from 5 to 4 mmol/L would increase your risk of dying by 400%.
"Elaine Meilahn reported in Circulation (2005) “In 1990, an NIH (National Institutes of Health) conference concluded from a meta-analysis of 19 studies that men and, to a lesser extent, women with a total serum cholesterol level below 4.2 mmol/L exhibited about a 10% to 20% excess total mortality compared with those with a cholesterol level between 4.2 and 5.2 mmol/L. Specifically, excess causes of death included cancer (primarily lung and hematopoietic), respiratory and digestive disease, violent death (suicide and trauma), and hemorrhagic stroke.” (Ref 3)
Refs
1 Schatz, Masaki, Yano, Chen, Rodriguez and Curb, “Cholesterol and all-cause mortality in elderly people from the Honolulu heart programme”, The Lancet, (August 2001).
2 Anderson, Castelli and Levy, “Cholesterol and Mortality: 30 years of follow-up from the Framingham Study”, Journal of the American Medical Association (JAMA), (1987).
3 Elaine Meilahn, “Low serum cholesterol: Hazardous to health?” Circulation, (2005).
@zor, an estimate of how many calories are in a pound of fat tissue is useful, in theory at least, for an endurance athlete who wants to know how long their energy reserves might be expected to last.
It is completely useless for predicting weight gained by eating or weight loss by exercise.
The conversion of carbohydrate to fat, for example, is so inefficient that most carb calories are expended in the conversion, 20% or less are saved as fat, and it is the insulin response to carbohydrate added to the energy contribution from carbohydrate and dietary fat together that determines fat storage – in the case that it does in fact happen.
Under such circumstances, no estimate is useful.
Zoe,
I am completely blown away by your statements. Especially in light of the fact that I have been told by my doctor that I need to lower my cholesterol levels and I am at the point where they want to put me on medications. Your contrarian data as well as the numerous studies you offered will be reviewed before I make any decision to go on medication to lower my numbers. I will also request that my doctor review some of the studies you cited and answer the question, why didn’t higher cholesterol numbers translate into more CVD.
Thanks for providing some additional insights that are eye opening.
I have thought about taking time off and then retesting; again, just out of curiosity but that would be “very difficult” for me to do. Training becomes almost an addiction even though I “hate” the pain of the sessions but then like the feeling afterwards. I have previously thought about seeing Dr Kendrick (I am close enough-ish) and think I may just do that. Thank you!
In terms of watching the footy for a month, do you really expect England to last that long?! ;)
Thanks also for publishing my posts – I half didn’t expect you to.
Hi again Mark. Ha ha! There are teams other than England playing! Wrong shaped ball for me anyway ;-)
If you can get a copy of today’s (Saturday’s) Times – there’s an interesting bit in an interesting article. I’ve cut and pasted the interesting bit: http://www.thetimes.co.uk/tto/health/diet-fitness/article4111188.ece
Dr Carl Lavie says: “But just as fat is not always bad, exercise is not always good. There have been many studies that show that the benefits of running can come to a screeching halt later in life. If you draw the blood of a person who has just run 26.2 miles in a marathon, about a third of them will have released the same enzyme that’s released in heart failure. If you do scans of their heart, about a third of them have dilation of the heart, particularly the right side of the heart. These abnormalities go away within days or weeks but it shows that this extreme level of exercise has some toxicity.
“So if somebody does a marathon and never does it again, even if they get the abnormality they’ll recover in a few days, but people who do this over and over again are risking chronic damage.”
About that footy!
Best wishes – Zoe
p.s. worth a session with Malcolm just for the entertainment value – so funny :-)
Hi Zoe
Thanks for your reply to my post below.
(I almost didn’t actually expect a reply because I’m aware that everyone shies away from making any form of diagnosis on the internet. I’m not after a diagnosis per se, but just a general discussion surrounding my “high” cholesterol levels which would probably drive most GPs for the statination pad…!
I’ve read “The Great Cholesterol Con” by Dr Kendrick and follow his blog as well as yours so was not overly concerned about my levels even though they’re “high”. My cholesterol test was actually a year ago. A more recent one was actually just over 10 with the ratios about the same as a year ago. I decided to do the tests privately just out of curiosity having followed a LCHF diet for about a year after reading Volek and Phinney’s “The Art and Science of Low Carbohydrate Living” and their training book as well. I train very, very intensely at national competition level. My interval training is mostly done to my absolute limits and my heart rate exceeds my theoretical max for most of my sessions. Following my switch to LCHF I gained a podium place at a recent national event. I won’t give the actual discipline but it’s one of the most intense cardiovascular events there is. Incidentally, I lost about 30lbs on the LCHF diet (I didn’t consider myself overweight but still shed about 4″ from my waist!) and have regained about 7lbs but that being mostly muscle I think / hope! I’m stronger than I ever have been.
My exercise sessions have recently begun to worry me though. I bought a blood ketone meter based on the recommendations of Volek and Phinney and then bought a blood glucose meter. The ketone level is fine (I often struggle to get into ketosis, probably because of eating too much protein) but the glucose level post exercise worries me but I’m not sure what is “normal” for my circumstances. Everything on the internet brings up discussions about diabetes.
Prior to a 5km or interval session my blood glucose is usually between 4.2 – 4.5. All good. Immediately after the session it can be between 9.5 – 10.5. It usually drops to around 5.5 – 6 within the hour. Is this response normal or am I pre-diabetic? I appreciate my liver is pumping out glucose to feed my muscles and it doesn’t know when the session will finish but should it be going as high as 10.5? Could my stressing my body through my training be causing my high cholesterol due to my body subsequently rebuilding itself?
My HbA1c was 5.3 and a recent blood homocysteine test was 4.9%.
I’d go to see my GP but after seeing my cholesterol levels I know exactly what he’d do and I don’t even want the discussion with him or being reported as being “awkward”!
I know from reading your blog and especially Dr Kendrick’s that you’d say “cholesterol is just a number”, but even with all that I’ve read you can’t help but worry… Apologies! ;)
Hi Mark – very interesting! My first thought it that what your body is trying to tell you is: what’s going on?! You know that what you’re doing isn’t natural but it’s what you do/your passion I guess, so there will be consequences. The key sentence for me was “Could stressing my body through my training be causing my high cholesterol due to my body subsequently rebuilding itself?” I would say so! Something needs to repair any damage that you’re doing with this very, very intense activity.
I can’t help beyond agreeing with your thought I’m afraid. When you do something abnormal all bets are off on what normal body responses should/could be. Dr Malc does private appointments – it could be worth exploring this as an option if you’re close enough? http://drmalcolmkendrick.org/
Don’t suppose you could sit on the sofa and watch the footy for a month?! ;-)
Best wishes – Zoe
Tom – the phrase “perhaps due to diseases predisposing to death” is speculation, not science. Reading between the lines, it sounds like “the results were not what we expected or hoped for, so we’re going to make something up to explain them away”.
Incidentally, I can’t see how Zoe’s blog is particularly beneficial to her bank balance. If making money was her motivation she would be writing “The Gogi Berry and Chia Diet”, or “Zoe’s Fat-Free Drop-a-Dress Size-in-Two-Weeks Diet” (500 calories a day). That’s what makes money.
Zoe-I have to take you up on some more of your selective reporting of data. I looked up the JAMA 1987 study (abstract below). You conveniently fail to mention that “Under age 50 years, cholesterol levels are directly related with 30-year overall and CVD mortality; overall death increases 5% and CVD death 9% for each 10 mg/dL.” Or the conclusion that “After age 50 years the association of mortality with cholesterol values is confounded by people whose cholesterol levels are falling—perhaps due to diseases predisposing to death.” i.e cholesterol level fall when people get sick from other causes leading to the finding that people with low cholesterol are more likely to die.
Come on Zoe try upping your game rather than your bank balance.
Under age 50 years, cholesterol levels are directly related with 30-year overall and CVD mortality; overall death increases 5% and CVD death 9% for each 10 mg/dL. After age 50 years there is no increased overall mortality with either high or low serum cholesterol levels. There is a direct association between falling cholesterol levels over the first 14 years and mortality over the following 18 years (11% overall and 14% CVD death rate increase per 1 mg/dL per year drop in cholesterol levels). Under age 50 years these data suggest that having a very low cholesterol level improves longevity. After age 50 years the association of mortality with cholesterol values is confounded by people whose cholesterol levels are falling—perhaps due to diseases predisposing to death.
Zoe, I would be interested to read your comments on the genetic condition Familial Hypercholesterolaemia (FH).I am one of the 1 in 500 who have it but refuse to take statins.
I have retained a print off of a blog from the pen of the wonderful Dr Kendrick which refers to an unpublished study in the Netherlands in which University students whose fathers had proven CHD before the age of 55 years were recruited. Age an sex matched controls were recruited from the same populations for each case. Results:
2 of 1089 students with family history of CHD had FH
4 of 1727 controls had FH.
Thus the prevalence of FH in both groups was not significantly different at approximately 1 in 500. Dr Kendrick’s conclusion was “The evidence that heterozygote FH is, of itself, a cause of atherosclerosis is unsatisfactory”. Does the genetic test tell us anything about anyone?
Hi Mike – Uffe Ravnskov dedicates Chapter 3 of Ignore the Awkward to FH and he is doing a paper on the condition at the moment. The last email I saw from him on this (yesterday) was requesting more full papers from friends and it said “I find more and more studies showing no association between LDL and CVD/atherosclerosis in these people.” Watch this space!
My personal view on FH is that it is merely a marker. The genetic defect manifests itself in LDL cell receptors being impaired from taking LDL lipoproteins from the blood stream and hence the LDL in the blood is high. The real harm is the fact that the cell didn’t get the contents of the LDL that it needed. The particularly high LDL in the blood just tells us there’s a problem.
Hope this helps for now
Best wishes – Zoe
you idiot zoe, in regards to your 3500 caloreis does not equal 1 lb… its an estimation you genius!!! you wasted your and our time with stupid calculations to show its 100 calories up or down get a life!
So, should I be worried?
Total Cholesterol: 9.1mmol/L
HDL : 2.27mmol/L
LDL : 6.4mmol/L
Triglyceride : 0.91mmol/L
I follow a LCHF diet.
Hi Mark – I think that cholesterol can be useful as a marker – never as a cause of anything.
This is higher than the actual (non statinated) average, which is c. 7 mmol/l. But then some people have cholesterol levels of 3 so some people ‘need’ to have cholesterol levels of 9 for 7 to be the average! It’s still on the normal distribution curve so the level in itself wouldn’t worry me. What’s interesting is what it might say as a marker. Where is this for you personally? If this is your first ever test then see what the next one says (because it’s inaccurate by up to 20% on tests anyway). If it’s higher than normal is that because you’ve not been in the sun? Are you injured? Have you had an op? Are you stressed? The cholesterol test can tell you something – especially as a comparator with other readings for you personally. Against some made up number of 5, produced by a committee with pharma interests, it’s irrelevant.
Hope this helps
Best wishes – Zoe
Zoe, I’ve noticed that most prostate supplements contain Beta-Sitosterol. I presume we should stay away from these supplements??
Hi Kathy
I kept it simple talking about sterols generally. Here’s a reference that may help – the short answer is – I would!
Best wishes – Zoe
Phytosterols are cholesterol-like molecules found in all plant foods, with the highest concentrations occurring in vegetable oils. They are absorbed only in trace amounts, but inhibit the absorption of intestinal cholesterol (Ostlund, 2002). The most commonly occurring phytosterols in the human diet are βeta-sitosterol, campesterol and stigmasterol, which account for approximately 65%, 30% and 3% of diet contents respectively (Weihrauch and Gardner, 1978).
Another fascinating article that provides a mechanistic explanation for the effect of phytosterols on longevity is Ratnayke, WMN (2000) Influence of Sources of Dietary Oils on the Life Span of Stroke-Prone Spontaneously Hypertensive Rats. Lipids, Vol. 35, no.4
Thanks Ed! Will check that one out :-)
Just done so – here it is for anyone else interested.