
Saturated fat & CHD in Europe
This post shows that, for all 192 countries in the world, for men and women, for CVD deaths and all-cause mortality, the HIGHER the cholesterol levels, the LOWER the death rate; the LOWER the cholesterol levels, the HIGHER the death rate. The Pearson correlation coefficient gets higher as we move from male CVD deaths to female CVD deaths to male all deaths to female all deaths.
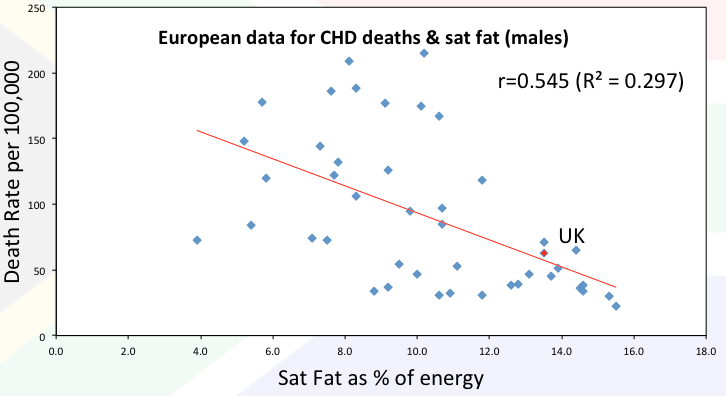
This blog repeats the exercise of examining the association between heart disease (this time CHD) and an accused causal agent (this time saturated fat). The data is available for Europe here [Ref 1]. As you can see below, the association is again inverse – the higher the saturated fat intake, the lower the CHD death rate for males…
and females…
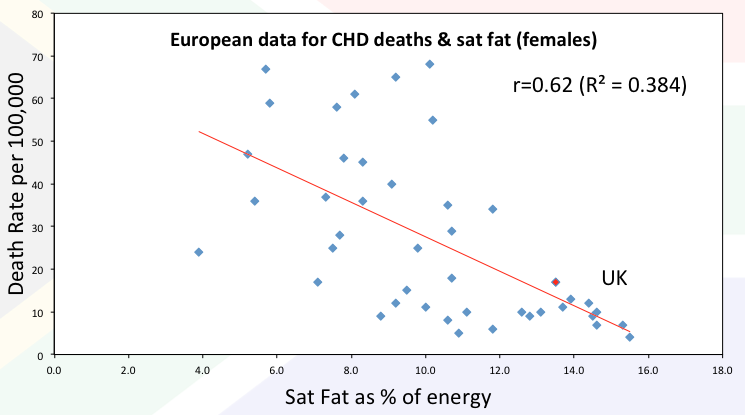
The correlation for males (r) is 0.545 and it is even stronger (0.62) for females.
The top and bottom seven
In the brilliant “The Great Cholesterol Con”, Dr Malcolm Kendrick reviewed the top and bottom seven countries for saturated fat intake in Europe and the countries with the highest and lowest levels of heart deaths. He used the MONICA data from c. 1998. I repeated this for the 2008 data [Ref 1].
* The 7 countries with the LOWEST saturated fat intake were Bosnia & Herzegovinia; Georgia; Azerbaijan; Tajikstan; Moldova; Croatia; Armenia.
Their saturated fat intake ranged from 3.9-7.3%. The average was 5.8% – all way below the recommended 10% saturated fat limit set by dietary guidelines.
* The 7 countries with the HIGHEST saturated fat intake were Austria; Finland; Belgium; Iceland; Netherlands; Switzerland; France (France is the single country with the highest saturated fat intake in Europe and the lowest rate of CHD deaths).
Their saturated fat intake ranged from 13.9-15.5%. The average was 14.7% – all way above the recommended 10% saturated fat limit set by dietary guidelines.
* The 7 countries with the LOWEST saturated fat intake had the following death rates:
– Male deaths per 100,000 ranged from 73-178, with an average death rate of 117.
– Female deaths per 100,000 ranged from 17-67, with an average death rate of 41.
* The 7 countries with the HIGHEST saturated fat intake had the following death rates:
– Male deaths per 100,000 ranged from 22-65, with an average death rate of 39.
– Female deaths per 100,000 ranged from 4-13, with an average death rate of 9.
Death rates for men were 3 times higher in the lowest saturated fat intake countries than the highest.
Death rates for women were 4.5 times higher in the lowest saturated fat intake countries than the highest.
As Malcolm found from the 1998 data – every single country in the top 7 saturated fat intake countries had a lower death rate than every single country in the bottom 7 saturated fat intake countries. This held for men and women. It holds again with the data from 10 years on.
The nutrition
Two facts are not widely enough known about fat/saturated fat and this explains much of the nonsense claimed about saturated fat. If people knew what saturated fat actually is, they would find their allegations about this life-vital nutrient as absurd as they are:
1) All food that contains fat contains all three natural fats (saturated, monounsaturated and polyunsaturated). There are no exceptions.
Meat, fish, eggs, dairy, nuts, seeds, olives, avocados – all of these foods contain all three fats. It is completely impossible to eat unsaturated fat without saturated fat, or vice versa.
2) The only food group that contains more saturated than unsaturated fat is dairy products. Meat has more unsaturated than saturated fat; eggs have more unsaturated than saturated fat; LARD has more unsaturated than saturated fat – not that any real fat is better or worse than any other – but just to set the record straight.
So – if you want a row about saturated fat – you’re having a row about dairy products and you may want to bear this in mind: There is evidence of a re-emergence of rickets and osteoporosis is rising [Ref 2]. The Family Food survey has reported that the present UK diet is deficient in retinol and vitamin D, providing less than one third of the UK Reference Nutrient Intake and barely a fifth of the recently revised American RDA for vitamin D [Ref 3].
As our 2013 paper suggests: “Using a 100 g steak, as an example, with 5.4 g of fat, it is difficult to accept that the 39% of the fat which is saturated is damaging to the cardiovascular system while the 61% of the fat which is unsaturated is protective. Keeping in mind that the total fat content of the steak will provide all but 3 of the 13 vitamins and 16 minerals that are a pre-requisite for the maintenance of good health.”
[Ref 1] Allender S, Scarborough P, Peto V, Rayner M. European Cardiovascular Disease Statistics: British Heart Foundation Health Promotion Research Group, 2008.
[Ref 2] S. H. Pearce and T. D. Cheetham, “Diagnosis and Management of Vitamin D Deficiency,” BMJ, Vol. 340, 2010, p. b5664. doi:10.1136/bmj.b5664
[Ref 3] DEFRA (The Department for Environment, Food and Rural Affairs), “A National Statistics Publication, the Family Food Survey,” The Department for Environment, Food and Rural Affairs, London, 2010.



Hello,
How can I get the raw data that you used to give this correlation? The links above are not working.
Hi Lisa
Check Ref 1 at the end of the article (Allender S, Scarborough P, Peto V, Rayner M. European Cardiovascular Disease Statistics: British Heart Foundation Health Promotion Research Group, 2008) Put this into a search box and the top result back should give you the chance to download the PDF.
Best wishes – Zoe
I don’t know if you’re still answering this thread, but why are the sat fat by country data not on the European cardiovascular disease statistics 2008 edition website?
Also, what do you make of this recent review by Mark Houston?
The relationship of saturated fats and coronary heart disease: fa(c)t or fiction? A commentary.
Ther Adv Cardiovasc Dis. 2018, Vol. 12(2) 33–37.
Excerpt: “SFA are diverse compounds, are not created equal, and cannot be ‘lumped’ into a single cate- gory. It is prudent to replace LCFA with PUFA, MUFA, whole grains, and dairy and plant proteins. The recommended grams per day, or percentage of SFA relative to total fat or total calories, cannot be accurately determined nor recommended at this time, but it is suggested that the SFA dietary intake should be well below 10% of the total caloric intake. (Mozaffarian D et al. Circulation 2015; 131: e29–e322). The overall relationship of the human diet to CHD should include the totality of our nutrition and avoid reductionist evaluations of single macronutrients. New nutritional guidelines should promote dietary patterns that improve CHD based on validated science.”
In my view, there is too much conflicting data on sat fat to make a conclusion. Even Salim Yusuf admitted that there may have too much confounding in the PURE study to accept the conclusion that sat fat has no effect on CVD except stroke.
Hi Bruce
I don’t know if they replace with more recent editions rather than keep the old ones or if they took the 2008 one off because we were able to do the graphs as in this post! They’ve never included the sat fat data again. I kept a copy of the 2008 PDF – Malcolm Kendrick wanted it recently, so we all know it exists!
On the other one – never look at one paper – especially an opinion piece. Look at the totality of the evidence as I have done here:
https://www.zoeharcombe.com/2018/03/the-us-dietary-guidelines/
and
https://www.zoeharcombe.com/2018/07/saturated-fat-consultation-sacn-my-response/
and
https://www.zoeharcombe.com/2018/05/sacn-report-on-saturated-fat/
and academic/peer reviewed papers as follows:
RCTs then: http://openheart.bmj.com/content/openhrt/2/1/e000196.full.pdf
Epidemiology then: http://bjsm.bmj.com/content/51/24/1737
RCTs now: http://openheart.bmj.com/content/openhrt/3/2/e000409.full.pdf
Epidemiology now: http://bjsm.bmj.com/content/51/24/1743
Finale (the one to read)
https://bjsm.bmj.com/content/51/10/769
Best wishes – Zoe
Hi Zoe,
Just came across your papers and youtube videos. Stirring content that is well presented.
I too was trying to find the raw data. I did manage to download the British data as you had mentioned.
The European data could not be found, would you be so kind to share the 2008 pdf “European cardiovascular disease statistics 2008 “?
I also run high cholesterol and most of my friends are on statins. Have been following you and Dave Feldman. I had my Carotid Artery Intima Media Thickness test done recently as was as Calcification score. If you know any other tests that would allow us to see the reality of our cardiovascular health I would love to know. I am South Asian and have a strong family history of heart disease. Most doctors in India only prescribe statins, which I refuse to take.
Hi Junior
Many thanks for your kind words. I know Dave well! He’s doing really interesting and original work.
Ivor Cummins is another one to search on youtube – he also has presentations from low carb Denver and other low carb conferences on open view. He’s Mr Calcification and other useful measures.
Dr Nadir Ali (cardiologist) is brilliant too https://lowcarbconferences.com/dr-nadir-ali-why-ldl-cholesterol-goes-up-with-low-carb-diet-and-is-it-bad-for-health/
I’ve found the 2008 PDF and will email it to you
Best wishes – Zoe
Isn’t lack of exercise a big risk factor for CHD?
Hi Johnny – yes – and smoking ahead of that and three things you can’t do anything about ahead of that. https://www.zoeharcombe.com/2014/05/heart-disease-the-facts/
It really has naff all to do with a natural fat found in all foods that contain fat!
Best wishes – Zoe
Excellent
Also interesting that top 7 & bottom 7 also roughly richest & poorest
Yes – Yerushalmy & Hilleboe spotted the GDP fat/heart connection back in 1957. Yudkin was there with his observed associations between cars/TV sets and heart disease!
Best wishes – Zoe
Hi Zoe,
Actually I stumbled upon this blog.
It happened to be a good thing! I am 47 yrs old and 3 yrs back I had an encounter with heart attack -Nothing serious now – The doctor gave me a choice. Stunt or medication. Since there was a choice, I opted medication. I have been taking Atrovastin 40mg, sorbitrate 10 mg and Clopitab A75 since then.
As I felt that I have been granted a second Chance, I have been very active since then. I have joined in a gym and working out regularly. But I am experiencing severe pain in the joints.mostly in elbow and shoulder. I presumed it to be gym injury. Recently heavy pain in my hip. Can’t bend forward. Have skipped the gym for the past 1 month.
Is it because of Atrovastin? And also avoided oily and fatty foods. In India, it is very hard!
Can you help me out. Since your blog was completely different from what I have been hearing from the doctors.
Is oil essential to the movement of the joints. (Lubrication).
Sorry if I am naive!
Hi Arun
Hopefully this post (and the links it connects to) will give you plenty to think about. https://www.zoeharcombe.com/2015/03/worried-about-cholesterol-andor-statins/
The joint pain you describe is exactly what I would expect from statins – surf around on forums of side effects and you’ll likely meet other people going through the same thing. What I’m saying is different to many doctors, but by no means all. A growing number are very anti-statins and pro real food and any real fat it contains. The link has recommended reading from other such doctors at the end. That’s just a few. I’m in a yahoo forum with over 100 docs/academics who all think heart disease has nothing to do with cholesterol. You may enjoy this set of blogs too – start at post I – it now up to post VII
http://drmalcolmkendrick.org/2016/01/18/what-causes-heart-disease/
Best wishes – Zoe
Pingback: People and Carbs in the Metabolic Syndrome Era | Jeff's Health Notes
Hello Zoe,
Much convinced about all this. Stopped Statins two months ago and feel much better.
My question: does porridge count as a cereal to avoid. I grew up on it and am a regular consumer, but can find nowhere, whether it is processed, a fast carb etc. Since I am only two kilos heavier than I was fifty years ago, it can’t be that bad.
Love your blog.
Hi Chris
Many thanks for your kind comment!
I’m quite a fan of porridge. For those who avoid all grains/starchy carbs, it’s a no, but I enjoy it regularly. It’s a better grain than wheat – in my opinion and Dr William Davis (Wheat Belly) and Dr David Perlmutter (Grain Brain) would agree! The non-wheat sucrose free cereals are mainly porridge and puffed rice cereal – the latter being more likely to disturb blood glucose levels.
There are processed versions – they’ve sprung up in high street coffee chains recently. There are speedy oat packets in supermarkets etc. Just get plain oats – cheaper, healthier etc.
You’re doing well with your weight!
Best wishes – Zoe
Please request a review of the study mentioned by Stephan Guyenet, http://wholehealthsource.blogspot.com.br/2015/04/new-study-strengthens-case-that-ldl.html
There really claim that this foundation high LDL is one of the leading causes of heart disease.
Thanks,
Rogerio
Hi Zoe
We LCHF followers agree saturated fat is not bad and has something very good for us. But science daily site today published new research that says the opposite for heart health.
http://www.sciencedaily.com/releases/2015/04/150427101527.htm?utm_source=feedburner&utm_medium=email&utm_campaign=Feed%3A+sciencedaily%2Fhealth_medicine+%28Health+%26+Medicine+News+–+ScienceDaily%29
I am wondering how we are going to respond to this amazing conflict???
Your words of wisdom would be interesting
Robert, Cape Town.
Hi Robert
Always start with common sense – would we have survived (indeed thrived) over 3.5 million years had nature/God put all the nutrients we need to live (essential fats, complete protein, vitamins and minerals) in the same foods that were trying to kill us (by containing saturated fat). If you were at the LCHF conference in Cape Town (no doubt!) you’d remember my slides about every food that contains fat contains all three fats (sat, mono and poly) – there are no exceptions. Hence we cannot eat one fat without eating all three (not in food anyway).
Here’s the article by the way: http://www.degruyter.com/view/j/ersc.2015.2.issue-1/ersc-2015-0004/ersc-2015-0004.xml?rskey=j49jnu
Just check this great line in the results and conclusion of the PDF:
Results: “Interestingly, co-administration of oleate with palmitate abolished cell death, and ER stress.”
Conclusion: “Importantly, the lipotoxic effects of palmitate are abolished with the co-administration of oleate.”
I have very little clue what the heck they are talking about and the detail of what they’ve done – to rodents note – but those two lines are gems…
The link you provided talked about olive oil, of course, known as it is for its high oleic content. Did you know olive oil is c. 7.5% – 20% palmitic acid? And the study found that – put them together and all is ABOLISHED! Love that word – pretty definitive. How clever is nature/God to design food that has all the right bits in the right proportions so that we don’t all drop dead.
Hope this helps!
Best wishes – Zoe
Thanks for your response appreciated
Yes I was at the conference – enjoyed it. We have exchanged blog comments before.
You too seem to have found this research a little confusing. I am reading you as saying that they seem to have shot themselves in the foot by that confusion???
Thanks Robert
Hi there – I’m sorry not to have made the connection – I quite often forget what I got up to do! Head too full :-)
Interesting one – you could see it as a foot shot. I see it as 99%+ of people do not know the basics about nutrients in food – fat especially. I think they have tested a classic saturated fat and a classic monounsaturated fat and just have no idea that they would be found together in some foods and are in olive oil. Had they known more about food nutrition they may have tested different actual foods on humans (on the basis that humans don’t isolate one chain length fatty acid from another – the caveat being that medium chain fatty acids are sometimes extracted for therapeutic purposes, but this isn’t food). I don’t see the point of testing something that humans wouldn’t eat in a natural diet and on rodents! Maybe any headline that bashes sat fat is a worthy end in mind in itself?!
Bye for now – Zoe
Zoe,
Love your research…….!, BUT,
Surviving 3.5 Million years? Really?
Now, I feel you are ” way off track” , getting into the “Great Debate of the Origin of Man ”
Naturalism vs. Creation” . As a Christian, I am blessed with your due diligence of “Science in Nutrition.”
Please…. keep up the good work..
Best,
Gary
dear Zoe,I am an eye MD with normal cholesterol levels and not obese,not a diabetic and hypertensive. but suffered a massive MI.I stopped statins after I read u r article.my hdl levels are less than 30mg/dl as for most Indians.if higher cholesterol levels indicate a lower mortality due to CVD please suggest measures to increase cholesterol levels.
Hi Satish – humans should no more try to increase cholesterol than lower it. We need to leave the body alone to make the cholesterol it is designed to make!
Best wishes – Zoe
Hi Zoe,
I have the following result:
Cholesterol 7.8
HDL: 1.75
LDL 5.37
Ratio 4.45
I’m 65, have a normal weight and blood pressure.
My doctor said to me today, apropos my refusal to take statins, “you will have a heart attack or stroke”. Not: “you might…”
She may be correct of course (well we have to go some way). She is sending me on to the hospital to let them argue the toss with me.
I’m very familiar with the arguments that you put forward and imagine though that I’ll be meeting entrenched interests.
One question I may struggle with is why I have a high cholesterol reading? Of course, why not? In any population there is a range. In your reading is there any proven negative association between having high a total cholesterol result and any health outcome?
Thanks for your work in this area.
Hi Nigel – hopefully the reply to Alex will help on this post with today’s date (20 March)
https://www.zoeharcombe.com/2012/06/why-hasnt-my-healthy-diet-cut-my-cholesterol/
You have the same (normal) cholesterol level and the same time of year and other points apply.
How dare your doc say this WILL happen?! If she’s that prophetic she can pick the lottery numbers for me tonight!
Best wishes – Zoe
I’m curious about the three factors which were stated to be largely responsible for heart disease and over which we have no control, namely: gender, age and genetics.
These factors have always been around, yet we’re told heart disease hasn’t until about the 1920s. How is that circle squared? Stress has equally always been around.
Hi Mark – interesting point. Almost all diseases were classified in the modern era – most in the 20th century. It doesn’t mean we didn’t suffer them before – we didn’t record them. Search pub med for ancient heart disease and 437 papers come up e.g. http://www.ncbi.nlm.nih.gov/pubmed/25667090
There is also the argument that we died of other things before the 20thC brought anti-biotics, vaccines, anesthetics and other medical advances. When we no longer die from being eaten by animals or from an infection caused by an every day injury or from flu or the plague – we live long enough to die of old age and the older we get, the more likely the heart is to pack up. The ultimate diagnosis of death in all of us is the heart stopping – what did we record this as before we recorded it as heart attack?
I think stress is very different now to what we have evolved to cope with. We have always had the stress of survival – get enough food and shelter to live and then anything on top is a bonus. This is still the stress for much of the world and it’s awful, but it’s all humans have known. The so called developed world largely has basic needs met but we have this alien world of technology and concrete and more people around us than the number who have died throughout history. Plus – we used to at least have the real food to cope with stress in pre-fake-food days. We now are expected to maintain a robust fright/flight/figh mechanism on Coco-pops!
Despite all the human (medical) advances that have helped, we humans have done some pretty stupid things to lose any advantage given!
Nice one
Best wishes – Zoe
I’m genealogy researcher and we can see in death records from houndreds of yours here in Sweden how heart diseases have exploded. The cause of the death are always writen down. CVD was writen down as bad heart. A lot of people died of “old age” or some of the viruses or in accidents. CVD was very rare before 1930 and all the other metabolic diseseases also. You can see CVD in mummies in china but only in rich people.
We’re often told not to look at surrogate markers which is all those papers can ever really point to. If we admonish big pharma for using this tactic then we can’t do it ourselves. An artery can be occluded up to and including 100% without a MI necessarily occurring. And it’s a fallacy to state that we’re living longer now than ever before. More of us may live through infancy so that skews the average somewhat.
I’d still therefore go with what I’ve previously read, that prior to the 1920s, heart disease was relatively rare to the extent that most doctors didn’t even recognise the symptoms.
I’d like to apologise if my last post came across a bit arrogantly or heavy handed – that wasn’t my intention.
I’m just not entirely convinced about the “we’re living longer now than ever before” slant that a lot of health reports seem to suggest. Arithmetic means, medians, ages weighted or otherwise, infant deaths etc can all skew figures.
If, however, we accept the paradigm that we are living longer than ever before then it’s an easy next step to say that: “that’s why we now have cancers, and heart attacks because well, we have to die from something and these diseases are all diseases of old age!” I don’t believe they are! I believe they are the consequences of eating the crap and rubbish which passes for food these days and also the epigenetic consequences of doing so. I suspect that in the past, a great majority of elderly people just expired, living fruitful, useful and fulfilling lives right up to the very end. And the reason I suspect this to be true is that they ate real food which nourished every single cell in their bodies, the way the body was designed to be nourished. So, natural, real food didn’t have to “protect” their arteries from occlusion because the natural, whole nutrients nourished the epithelium and kept it healthy from an early age. Their brains didn’t get “short circuited” as in many people today resulting in Alzheimers’ or other dementias (or ADD / ADHD in kids) because the copious fats they weren’t afraid of consuming together with naturally occurring B vitamins and B12 in real food nourished their brains for life.
And this is why I refuse to take part in or support the, “let’s beat cancer” or “heart disease” “charities” in their “fighht back” campaigns. We aren’t going to beat cancer or heart disease because the “fight back” is entirely misguided (however well intentioned) and will never succeed. Beating cancer or heart disease or dementia doesn’t require a “fight”, it simply requires good old fashioned real food from day 1. The epigenetic inheritance is then passed onto future generations.
But there’s no money in real food or even in supplementation, is there?
Hi Mark – you didn’t come across that way at all – it was one of the best points made. Plus I think we agree on everything! I agree with you on the impact of infant mortality and that those who did survive this/infections/accidents etc lived as long as people today. I also agree with you on the real food – that’s my single motto for eating advice. I also agree with you on ‘health charities – not yet come across any of a decent size that are independent of conflict with drug/fake food companies (the small ones set up by family/friends in someone’s memory tend to be honest if they stay small). And I agree on the final sentence!
One of my prof supervisors thinks epigenetics are going to answer way more things than we currently realise – so he’ll agree with you on that :-)
Best wishes – Zoe
Wallace and Grommit were right after all. CHEESE.
I loved Ludkin’s work, and to really nail the lid shut on the saturated fat- cholesterol – heart disease hypothesis, epidemiology on sugar intake is crucial. From memory, Malcolm commented that the humble Australian Aborigine had a 100x heart disease risk. I love the factoid that Coca Cola admitted that the highest sales of Coke any where in the world was- Australia’s Northern Territory. Even the “dry” (no alcohol) communities are being sucreminated (my neologism) by the white stuff, which is sold by the bucketload.
Hi, Zoe!
Thank you for great information. My husband and I started low-carb diet recently. One thing about higher saturated fat intake that makes me nervous and that I don’t seem to find information for is how it may affect recurrence of breast cancer. I read that there was a study proving that higher saturated fat intake is linked to a higher recurrence rates. Do you have an opinion or data about that?
Thank you!
So many questions, so little time…
I’m curious how an adjustment for medical care would affect the graphs, as the wealthier countries (which also tend to eat more sat fat, it seems) would be better able to reduce death rates from CHD by intervention. I think it might explain that “shelf” effect in the charts, where variance drops drastically as sat fat % > 12.0%. That is, if those high-fat countries are all wealthy and have good care, then they’re possibly reducing CHD death by *both* diet and intervention.
Below 12%, I’m really curious if the low-CHD-death-rate countries have better medical care than the high-rate ones.
So many other interesting things in that report, though. Greece, for example, is the highest fruit/veggie eater and also has the highest obesity problem (though that doesn’t hold for, say, Poland). You can also identify the Iron Curtain in many of those figures. On page 67, it also notes that poorer countries likely have higher fruit/veggie consumption than the study reports since they rely more on personal gardens (which aren’t included or accounted for).
Good info!
Hi David – such confounders are alternative hypotheses. Smoking cessation and emergency care (the critical first 5 mins) have been major drivers of reductions in heart disease/heart deaths in the past 20-30 years. Both are reflections of health care policy and practice. Does health care cause heart outcomes? Absolutely. The more confounders that stand up to scrutiny the better, because it isn’t sat fat driving heart disease!
Best wishes – Zoe
Seems like a super-easy way to remove the divergent health care system confounder would be to look at CHD _incidents_ rather than deaths. CHD incidents will reflect a country’s diet/lifestyle. Deaths is a black-box interaction between diet/lifestyle and health care system. CHD Deaths are such an obviously confounded number that I honestly have started seeing these graphs as a red flag of someone practicing shady statistics. Can you give us this graph again with incidents? Or is that information not available in a consistent way for enough countries?
Hi Alicia
The source is posted in the article. On p38 there is data for coronary events but not such that can be matched with sat fat intake in many cases. The event data is for the MONICA cohorts – more than one entry for each country in many cases, which is interesting in itself. Finland has 3 cohorts ranging from (male) coronary events of 549 to 835 per 100,000. Same healthcare system. France has 3 cohorts also – ranging from (male) 233 to 298 coronary events per 100,000. France still has the highest sat fat intake in Europe – which – remember – is what the post is about.
I like your thinking though because CHD incident/deaths will have some causes – it’s just that sat fat isn’t one of them.
The three main causes we can do nothing about: age, gender, genetics https://www.zoeharcombe.com/2014/05/heart-disease-the-facts/ (male death rates are 3.4 times those of females for all the European countries).
Best wishes – Zoe
Anecdotally, the Greeks serve and eat huge portions, particularly of chips. A popular lunch is one or two Greek style chip butties – kebab cones stuffed with chips. And a side order of fries in a restaurant is massive.
Zoë / Jonathan, I appreciate both responses. I didn’t know about Greek portions and fondness of chips. Learn something new every day. Thanks!
I lived in Greece for many years and im afraid those “butties” are for the tourist’s.
Greek’s eat lots of fish/meat/salad and olive oil.
Excessive chips in greece is a “modern” thing …remember it started 30’sh year ago. After I left
David Hooper
The report Zoe used also provides data on the availability/use of “Fruit&Veg”. Several years ago I regressed this data against the national incidence of CHD just as done above for fat. “Fruit&Veg” too was significantly and negatively associated with heart disease, ie more “Fruit&Veg”, less CHD. Interestingly, this set of reports ignored carbohydrate; the authors used the word once to say it was good. Unfortunately, the estimated availability of carbohydrate (100% – “Fruit&Veg” – fat – protein) was significantly and positively associated with CHD incidence. Another example of bias and selection to support the “Food Gospel”
Thanks. I can certainly believe that. Not all carb sources are equal, for sure.
Well this is really encouraging, since I’m a woman and many of the foods I like best are full of saturated fat- (cheese, cream, liver pate, macadamia nuts, coconut oil….) This reminds me, I thought coconut and coconut oil were the foods highest in saturated fat?
And thanks for reminding everyone that all foods with fat contain all 3 fats; I think many people forget this, even nutritionists.
A propos dairy products: I’ve read about some studies that confirm that people whose diets are high in cheese and other dairy products have a lower rate of heart disease, presumably- (at least partly) due to the high vitamin K2 content, which is protective. I don’t remember where I’ve found that, but I’ve read about it in a couple of different publications recently (I could probably find them again if need be).
Hi Lisa – coconut oil is the single highest source of saturated fat – I emphasised food GROUP. Dairy products are the food group with more sat than unsat fat. Oils as a group vary depending on the oil – olive oil higher in mono; sunflower oil higher in poly, coconut oil higher in sat – but they all have all three fats! When people say animal fats are saturated and plant fats are unsaturated, they show their ignorance.
I stuck dairy heart disease (review, meta-analysis and/or systematic review) into pub med and there are over 500 articles. This was one of the most relevant: http://www.ncbi.nlm.nih.gov/pubmed/25476191
There is plenty of evidence that dairy products are healthful, not harmful. A simple analysis of all nutrients (not just K2) will explain why.
Best wishes – Zoe
Great to have this info. Cholesterol levels vary hugely among people and there doesn’t seem to be a link between cholesterol and cvd. Dr Kendrick does think however that stress (and associated chronically elevated cortisol Ievels) is responsible – not diet. What is your view on this?
Hi Audrey – I think that the three main factors in heart disease we can do nothing about: gender; age and genetics (https://www.zoeharcombe.com/2014/05/heart-disease-the-facts/).
The number one factor we can do something about is smoking – don’t! I agree with Malcolm that other things that can damage the endothelial wall can cause heart disease – stress, sugar, adrenal/cortisol exhaustion etc. We (conveniently) forget the big three that we can do nothing about however – it doesn’t help fund raising.
Best wishes – Zoe