
SACN report on lowER carb diets for T2D

Executive Summary
* In March 2020, SACN, the UK Scientific Advisory Committee for Nutrition, invited submissions for a consultation about lowER carbohydrate diets for adults with type 2 diabetes (T2D). I submitted a response, which is included in this note.
* The final report has just been published. It concluded that a lowER carb diet can be recommended by clinicians as a short-term option.
* There were five flaws with the consultation document, which have not been addressed:
Flaw 1 – The committee members have conflicts of interest in favour of low-fat high-carb diets. Most members have established (and largely unfavourable) views on low-carb diets.
Flaw 2 – The rational for the review was given as Public Health England asked us to review this because low-carb diets are increasingly being promoted. The committee then rejected the evidence from the physicians and academics promoting these diets.
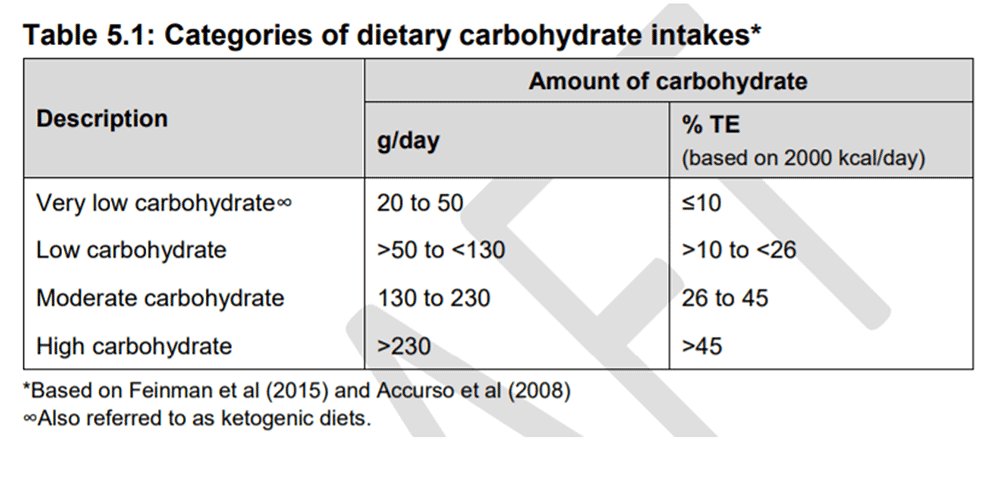
Flaw 3 – Examining lowER vs low is a significant flaw. The committee members showed that they know the definition of low carb, but then did not study low carb. LowER carb was carbohydrate comprising 13-47% of total energy and highER carb was 41-55% of total energy. They overlapped.
Flaw 4 – The report contained a section on carbohydrates, which showed that the committee knows that all foods that contain carbohydrate contain glucose and that glucose is the issue for people with T2D and yet they continue to favour high-carb diets.
Flaw 5 – If only the same bar had been set for the introduction of low-fat, high-carb guidelines. The rationale for only recommending low-carb diets in the short term (“up to 6 months”) was given as – we don’t know the long-term implications of lowER carb diets. We do know the long-term implications of low-fat diets and they are serious and yet these are still recommended.
* This is too serious an issue for a committee to be reticent to advise people who can’t handle glucose to avoid glucose – and long term.
Introduction
On March 5th, 2020, Public Health England announced, “We are seeking scientific comments on SACN’s draft report: ‘Lower carbohydrate diets for adults with type 2 diabetes’” (Ref 1) SACN stands for Scientific Advisory Committee on Nutrition. This is the body tasked with reviewing dietary policy for Public Health England.
Health was devolved in the UK in 1999, so that England, Scotland, Ireland and Wales all have their own public health bodies and chief medical officers. However, when it comes to diet, the regions tend to follow England’s lead and thus anything decreed by SACN ends up being UK wide policy.
The draft document was dated January 2020, but the invitation wasn’t issued until March 5th and the deadline was April 30th, 2020. I wrote a Monday note on April 13th, 2020, about the remit and conflicts of interest of the SACN committee (Ref 2). I also shared the planned method and the evidence that was being considered. The committee chose to focus on systematic reviews and meta-analyses, as best evidence. The primary outcomes of interest were body weight ≥ 12 months and HbA1c ≥ 3 months (HbA1c being the measure of blood glucose levels for the past 3 months).
I submitted my response on April 26th, 2020. My response forms a major part of this note.
The final report has just been published (May 26th, 2021) (Ref 3). Medscape reported the conclusion with rather more of a positive twist than the report might have liked “Committee on Nutrition Recommends Low-carb diet for Type 2 Diabetes” (Ref 4).
The recommendations were summarised in the report in paragraphs S25-S29. The report said, "For adults living with T2D and overweight or obesity, a lower carbohydrate diet can be recommended by clinicians as an effective short-term option (up to 6 months) for improving glycaemic control and serum triacylglycerol concentrations." The caveats were many – the recommendations were only for adults living with T2D and overweight or obesity and only for up to 6 months.
Low vs LowER carbohydrate
One worry from the outset was that this report would become the definitive position on low-carb diets, even though it hasn’t studied them, and never set out to study them. The opening summary confirmed this concern.
The title of the report remained “Lower carbohydrate diets for adults with type 2 diabetes.” The first two points in the summary, however, referred to ‘low’ carbohydrate diets (references to Sx are paragraph numbers in the final May report, in case anyone is interested).
“S1 The purpose of this report was to review the evidence on ‘low’ carbohydrate diets compared to current UK government advice on carbohydrate intake for adults with type 2 diabetes (T2D).
“S2 It was initiated in response to a request from Public Health England, for a systematic assessment of the scientific evidence on ‘low’ carbohydrate diets, in recognition that such diets are increasingly being promoted.”
Summary point S4 argued “Since there is no agreed and widely used definition of a ‘low’ carbohydrate diet, comparisons in this report were between lower and higher carbohydrate diets.” I disagree that there is no agreement on what a low-carbohydrate diet is. The committee shared (Feinman) definitions of low carbohydrate in the draft report, and these definitions can be agreed upon (they are in the low-carb world). I addressed this in Flaw 3 in my submission.
The report concluded that it was not possible to compare ‘low’ and ‘high’ carbohydrate diets for the primary outcomes because the definition of a low-carb diet varied widely across randomised controlled trials (RCTs) (S14). The definition does vary, but that did not preclude the committee from setting the correct definition of low and high carbohydrate and measuring RCTs that fell into these categories. Instead, carbohydrate intakes in “lower carbohydrate groups” ranged from 14 to 50% of total energy, which is absurd. I don’t know anyone prescribing low-carb diets for T2D who would go anywhere near as high as 14%, let alone 50% carbohydrate. Perhaps even more absurd, there was also overlap in carbohydrate intakes between the lower (13 to 47% of total energy) and higher (41 to 55% of total energy) carbohydrate diets, when reviewed together. The report said “Comparisons, therefore, were largely between lower and higher rather than ‘low’ and ‘high’ carbohydrate diets.” The reality is that comparisons were between absurd categories (S15).
Results
Despite this, lowER carb still did best. The report concluded, “Overall, the evidence suggests beneficial effects of lower carbohydrate diets on HbA1c, fasting plasma glucose and serum triacylglycerol in the shorter term (up to 6 months)” (S16). The report also concluded that there were no differences between higher and lower carbohydrate diets on total cholesterol or LDL cholesterol either in the shorter (≥3 to 6 months) or longer (≥12 months) term (S19).
But then we got the kicker that we always get (S13) “The implications of longer-term (≥12 months) restriction of carbohydrates in adults with T2D are currently unknown due to a lack of data from longer-term intervention studies.” We had absolutely no idea of the implications of a low-fat high-carb diet when we changed dietary advice in the late 1970s/early 1980s, but that didn’t stop us doing it. We arguably have decades of evidence that this has been disastrous, but this hasn’t stopped us reiterating this dietary advice. I addressed this in Flaw 5 in my submission.
I must mention the finding reported in S29: “Adults living with T2D and overweight or obesity who change to a lower carbohydrate diet and are taking diabetes medication may be at risk of hypoglycaemia. It is recommended that they receive advice and support from their health care team to manage this risk and to make adjustments to their medication as required.” i.e., if you lower carbs you will lower blood glucose and you will need lower meds. Isn’t this the entire objective? And that’s only with lowER carb – you want to see what low carb can do!
My submission
I’ve included my submission in full because it still holds. The clause and page numbers below refer to those in the 2020 draft report for consultation, but you shouldn’t need to refer to that draft report. You’ll understand the points being made…
———————–
There are five fundamental flaws with this review and the process should be stopped until they have been addressed:
Flaw 1 – Conflicts of interest.
As is a feature of SACN committees, there are conflicts of interest among panel members (p5) (Ref 5).
a) Food and pharmaceutical organisations.
One of the co-chairs and two other panel members have conflicts of interest with the International Life Sciences Institute (ILSI). Their members are a who’s who of the fake food industry/manufacturers of processed carbohydrates including Coca-Cola, General Mills, Hershey, Kellogg’s, PepsiCo, Red Bull and many more (Ref 6).
One of the co-chairs also has conflicts with the British Nutrition Foundation – another body representing the fake food industry/manufacturers of processed carbohydrates. British Nutrition Foundation members include British sugar, Coca-Cola, Cargill, General Mills, Kellogg, Mars, McDonalds, Nestle, Pepsi, Tate & Lyle sugar and many more (Ref 7).
Other panel conflicts include Unilever, Mars, American Association of Cereal Chemistry International, Nestle, World Sugar Research Organization (more carbohydrate conflicts) and Amgen, Bayer, and Lilly (pharmaceuticals to counter the effect of carbohydrates).
b) The SACN carbohydrate review.
One of the co-chairs and another panel member were on the SACN review “Carbohydrates and health” (2015) (Ref 8). This concluded “It is recommended that the dietary reference value for total carbohydrate should be maintained at an average population intake of approximately 50% of total dietary energy.”
An example of the bias that this leads to is captured in Clause 5.42 – just below Table 5.1 which defines low-carbohydrate diets (see below). Clause 5.42 states “According to the above categories of carbohydrate intake, government recommendations on carbohydrate intake for the general population (50% of TE) would be classified as high.” Yes – that’s the point. This is not the panel to overturn its own guidelines.
c) Diabetes UK.
Half the panel are employed by, research for, or have other conflicts with Diabetes UK. The official dietary advice from Diabetes UK is still low fat/high carbohydrate dominated. Diabetes UK published a position statement on low-carbohydrate diets in May 2017 (Ref 9). Their position statement can be summarised as: begrudgingly supporting low-carbohydrate diets in the short term only; issuing cautions about safety; and thinking that lowering blood glucose is an issue rather than a highly desirable outcome.
Clause 3.20 and Table 3.1 sets out the Diabetes UK position. Table 3.1 summarises the current position among the peers of Diabetes UK and thus sets as a foundation the belief that carbohydrates should be 45-60% of intake, fat should be less than 35% and protein should be no more than 20%. With half the panel conflicted with Diabetes UK, this, again, is not the panel to overturn its own guidelines.
The draft SACN report is dated January 2020 and so Clause 3.20 should have captured the US consensus report published in May 2019 (Ref 10). This report examined low-carbohydrate diets (26-45% of total calories) as well as very low-carbohydrate diets (20-50g of carbohydrate a day). Both diets were reported to reduce HbA1c, deliver weight loss, lower blood pressure, and improve the lipid profile. The US consensus report did not caution that (very) low-carbohydrate diets were only safe and effective in the short term. The US consensus report did not use isolated papers to issue unnecessary safety concerns. The US consensus report contained 345 references. It went as far as to advise eating non-starchy vegetables.
Further example of bias was shown in the reporting of adverse events. Two of the systematic reviews (SRs)/meta-analyses (MAs) did not report on adverse events. One reported that the most serious adverse event was in the higher carbohydrate diet (clause 6.200). None of the 13 primary RCTs, included in the SRs with MAs, which reported on adverse events reported any serious adverse events related to the diet (clause 6.204). This did not stop the draft report noting “All 4 SRs with MAs observed the potential of carbohydrate-restricted diets to detrimentally impact CVD risk markers.” (Clause 6.203). Furthermore, despite the 4 chosen studies and 13 primary RCTs providing no evidence of harm, the SACN panel added their own comments in a section called “Potential long-term concerns.” The first comment in this section (clause 6.206) stated “The implications of long-term restriction of carbohydrates in adults with T2D are currently unknown since there is a lack of data from longer-term studies.” (See Flaw 5).
The review started off with confirmation bias and thus we can have no expectation of a genuinely independent outcome (Note 11).
Flaw 2 – Not addressing what the review set out to address.
The opening clause, Clause 1.1, stated: “The purpose of this report is to review the evidence on lower carbohydrate diets compared to current UK government advice for adults with type 2 diabetes (T2D). It was initiated in 2017, in response to a request from Public Health England (PHE), in recognition that such diets are gaining attention and increasingly being promoted.”
I am not aware of anyone promoting lowER carbohydrate diets for T2D. I am aware of a number of academic and medical doctors, in the UK and US especially, researching, publishing academic papers about, and promoting very low-carbohydrate diets (and low-carbohydrate diets as an upper, not lower, limit) – definitions in Table 5.1 below.
Clauses 5.9 and 5.10 are remarkable.
– Clause 5.9 opens with: “A number of clinical studies (including Saslow et al (2017); Bhanpuri et al (2018); Hallberg et al (2018), Athinarayanan et al (2019)) and case reviews (Unwin & Tobin, 2015) have assessed the effectiveness of lower carbohydrate diets on glycaemic control and other markers in adults with T2D” (Ref 12).
– Clause 5.10 then states: “These studies were not considered in this report because of the number of limitations associated with this study type. They also did not meet the inclusion criteria for study selection.”
These clauses effectively state, “we’ll set the inclusion criteria and then we’ll dismiss – in two paragraphs – all evidence from the genuinely low-carbohydrate doctors and academics.” There were more publications not even cited and dismissed. These are in my EndNotes, just as examples (Ref 13). There will be many more still if the panel were minded to look for them.
Facing a crisis of the scale that Type 2 diabetes presents, you would think that any and all evidence would be welcomed with open arms. It would seem not.
Flaw 3 – The decision to not study low-carbohydrate diets.
a) The SACN draft report shows that it knows what low and very low-carbohydrate diets are…
… and yet it has then chosen to ignore them.
It is worth noting that the very low-calorie DiRECT diet was a low-carbohydrate diet. It provided 825-853 kcal/day, of which 59% was carbohydrate, thus providing 122-126g of carbohydrate a day (Ref 14). That’s low carbohydrate in Table 5.1 above. DiRECT was thus low carbohydrate and very low calorie and yet no concerns about its safety were issued in the draft report.
b) Clause 6.2 informs us that just four systematic reviews with meta-analysis were used to provide the entire evidence in the SACN draft report. Normally SRs with MAs would provide the best evidence available, but the goal of this review was ostensibly to review the growing interest in (very) low-carbohydrate diets, and this evidence is gathering at the current time – to ignore all of this is to render the draft review pointless.
c) Earlier evidence was also ignored in the draft report (2008). Clause 3.13 states “Currently, there is no cure for T2D but data from dietary weight management programmes and bariatric surgery confirm that weight loss can result in remission (Diabetes UK, 2018b).”
In 2008, Dr Eric Westman et al published “The effect of a low-carbohydrate, ketogenic diet versus a low-glycemic index diet on glycemic control in type 2 diabetes” (Ref 15). The latter was a randomised controlled trial which randomised people to either a ketogenic diet (<20g carbohydrate daily) or a reduced calorie diet (500 cal deficit). The ketogenic diet achieved significantly better results for HbA1c, body weight, and reduction/elimination in diabetes medications. This provided evidence, back as far as 2008, that a genuinely low-carbohydrate diet can put T2D into remission – the authors used the phrase “reversing”, rather than remission, in the abstract.
The Feinman et al paper (Ref 16) should have been used in the draft report for all of its evidence – not merely for the definitions of low-carbohydrate diets. As the abstract summarises: “Here we present 12 points of evidence supporting the use of low-carbohydrate diets as the first approach to treating type 2 diabetes and as the most effective adjunct to pharmacology in type 1. They represent the best-documented, least controversial results. The insistence on long-term random-controlled trials as the only kind of data that will be accepted is without precedent in science. The seriousness of diabetes requires that we evaluate all of the evidence that is available. The 12 points are sufficiently compelling that we feel that the burden of proof rests with those who are opposed.” (My emphasis).
d) Table 6.1 summarised the “carbohydrate intake comparisons” in the four studies forming the entire basis for the SACN draft report. In what follows, TE is total energy:
Huntriss et al (2018) – “low carb diet must have achieved lower carbohydrate intake than the control group.” (That was it – just lower – no amount specified).
Korsmo-Haugen et al (2018) – “Diet <40% TE versus diet >40% TE from carbohydrates.”
Sainsbury et al (2018) – “Diet ≤45% TE versus diet >45% TE from carbohydrates.”
Van Zuuren et al (2018) – “Diet ≤40% TE from carbohydrates versus low fat diet (≤30% TE).”
LowER carbohydrate really does simply mean just lowER in carbohydrate than the other diet. Below 45% vs above 45% of carbohydrate intake. That’s all it needs to mean. The entire review is nonsensical. This was reported as a limitation of the SACN review (clause 6.62). It should have been reported as a fatal flaw.
e) Notwithstanding that low-carbohydrate diets were not studied, lowER carbohydrate diets performed better in the significant findings:
HbA1C. At 3 and 6 months, there were significantly greater reductions in HbA1c in the lower compared to the higher carbohydrate group. The evidence was graded as adequate. (Clause 6.130)
Fasting plasma glucose. In shorter-term studies (3-12 months), there was a greater reduction in fasting plasma glucose in the lower carbohydrate group. The evidence was graded as moderate. (Clause 6.140)
Triacylglycerol. Greater reduction in triglycerides in the lower carbohydrate diet in shorter-term studies (3-12 months). The evidence was graded as adequate. (Clause 6.163)
Imagine what results could have been achieved with a proper review of very low-carbohydrate diets (low carbohydrate as an upper limit)?
Flaw 4 – The absence of common sense.
The clauses “classification of carbohydrates” (section 2.2) inform us that:
i) glucose is one of the three main monosaccharides;
ii) glucose is present in fruit and milk (glucose is present in all three disaccharides);
iii) starch is “a polysaccharide of glucose monomers.”
This section confirms that every food that contains carbohydrate contains glucose.
Clause 3.1 states “Diabetes is a condition in which the body does not produce sufficient insulin to regulate blood glucose levels and the insulin produced does not work effectively. This leads to elevated blood glucose concentrations which causes damage to blood vessels and nerves.”
Clause 3.7 states “Diagnosis of T2D is on the basis of elevated blood glucose concentrations…”
Clause 3.8 states “Elevated blood glucose concentrations over time can have serious long-term consequences such as heart attacks, strokes, kidney diseases, blindness, lower-limb amputations and premature death.”
If diabetes is a condition in which the body cannot regulate blood glucose levels and raised blood glucose levels are catastrophic, why would diabetics be advised to consume the majority of their diet in the form of carbohydrate – the only macronutrient to provide glucose?
Flaw 5 – if only the same bar had been set for the introduction of low-fat high-carbohydrate guidelines.
Clause 5.1 informed us that only “evidence provided by systematic reviews (SRs) with meta-analyses (MAs)” will be considered and only from RCTs (clause 5.2).
Clause 6.206 stated “The implications of long-term restriction of carbohydrates in adults with T2D are currently unknown since there is a lack of data from longer-term studies.”
The implications of long-term restriction of fat (and concomitant increase in carbohydrates) in all adults was unknown at the time of the introduction of precisely these dietary guidelines (1977 US/1983-84 UK).
My PhD was an examination of the evidence base (using only systematic review and meta-analysis) for the introduction of the low-fat (high-carbohydrate) guidelines. There was no evidence at the time these guidelines were introduced from SR and MA of RCTs (Ref 17). (There was no evidence from cohort studies either (Ref 18)) There has been no more evidence from SR and MA of RCTs since (Ref 19). We had no idea of the implications of long-term restriction of fat (and concomitant abundance of carbohydrate) and yet we introduced these dietary guidelines anyway.
It would appear that the bar to change the guidelines (back to where they were) is substantially higher than the zero-bar applied to their introduction.
Summary
In summary, there are five fundamental flaws with this review and this review should be stopped until they have been addressed. Otherwise, this draft report risks becoming the official position on T2D and low-carbohydrate diets (the semantics of lowER will soon be lost) and that would be a travesty. The review requires:
1) An independent panel with no conflicts of interest.
2) Examination of the actual diets gaining attention, as the review claimed it set out to address.
3) Genuine study of very low-carbohydrate diets (low-carbohydrate diets as an upper limit).
4) Some common sense.
5) Some humility and acknowledgement of how low the bar was set to get us into a public health crisis of obesity and type 2 diabetes and how high the bar has been set to get us out of this. And then an acceptance of the Feinman et al position: The seriousness of diabetes requires that we evaluate all of the evidence that is available. The 12 points are sufficiently compelling that we feel that the burden of proof rests with those who are opposed.
References
Ref 1: https://www.gov.uk/government/consultations/lower-carbohydrate-diets-for-adults-with-type-2-diabetes-draft-report?
Ref 2: https://www.zoeharcombe.com/2020/04/sacn-consultation-on-lower-carb-diets-t2d/
Ref 3: https://www.gov.uk/government/publications/sacn-report-lower-carbohydrate-diets-for-type-2-diabetes
Ref 4: https://www.medscape.com/viewarticle/951881
Ref 5: https://assets.publishing.service.gov.uk/government/uploads/system/uploads
attachment_data/file/841591/SACN_Register_of_Interests_v21.pdf
Ref 6: https://ilsina.org/about-us/membership/
Ref 7: https://www.nutrition.org.uk/aboutbnf/corporate/memberorganisations.html
Ref 8: https://assets.publishing.service.gov.uk/government/uploads/system/uploads
/attachment_data/file/445503/SACN_Carbohydrates_and_Health.pdf
Ref 9: https://www.diabetes.org.uk/resources-s3/2017-09/low-carb-diets-position-statement-May-2017.pdf
Ref 10: Evert AB et al. Nutrition Therapy for Adults With Diabetes or Prediabetes: A Consensus Report. Diabetes Care 2019. https://care.diabetesjournals.org/content/diacare/42/5/731.full.pdf
Note 11: The SACN response to me saying they were conflicted was to reply that they have declared their conflicts (I know – that’s where I got them from) and so if they are declared, they are no longer an issue. That’s like saying Jeffrey Epstein has declared his interest in young girls, so he’s fine to work at a school!
Ref 12: Saslow LR et al. Twelve-month outcomes of a randomized trial of a moderate-carbohydrate versus very low-carbohydrate diet in overweight adults with type 2 diabetes mellitus or prediabetes. Nutr Diabetes 2017.
Ref 13: Unwin D, Unwin J. Low carbohydrate diet to achieve weight loss and improve HbA1c in type 2 diabetes and pre-diabetes: experience from one general practice. Practical Diabetes 2014.
Unwin DJ et al. A pilot study to explore the role of a low-carbohydrate intervention to improve GGT levels and HbA1c. Diabesity in Practice 2015.
Saslow RL et al. Outcomes of a Digitally Delivered Low-Carbohydrate Type 2 Diabetes Self-Management Program: 1-Year Results of a Single-Arm Longitudinal Study. JMIR Diabetes. 2018.
Unwin DJ et al. Substantial and Sustained Improvements in Blood Pressure, Weight and Lipid Profiles from a Carbohydrate Restricted Diet: An Observational Study of Insulin Resistant Patients in Primary Care. International Journal of Environmental Research and Public Health. 2019.
Saslow LR et al. A Randomized Pilot Trial of a Moderate Carbohydrate Diet Compared to a Very Low Carbohydrate Diet in Overweight or Obese Individuals with Type 2 Diabetes Mellitus or Prediabetes. PLoS One. 2014.
Evert AB et al. Nutrition Therapy for Adults with Diabetes or Prediabetes: A Consensus Report. Diabetes Care. 2019.
McKenzie LA et al. A Novel Intervention Including Individualized Nutritional Recommendations Reduces Hemoglobin A1c Level, Medication Use, and Weight in Type 2 Diabetes. JMIR Diabetes. 2017.
Ref 14: Lean MEJ, Leslie WS, Barnes AC, et al. Primary care-led weight management for remission of type 2 diabetes (DiRECT): an open-label, cluster-randomised trial. The Lancet 2017.
Ref 15: Westman EC et al. The effect of a low-carbohydrate, ketogenic diet versus a low-glycemic index diet on glycemic control in type 2 diabetes mellitus. Nutrition & metabolism 2008.
Ref 16: Feinman RD, Pogozelski WK, Astrup A, et al. Dietary Carbohydrate restriction as the first approach in diabetes management. Critical review and evidence base. Nutrition (Burbank, Los Angeles County, Calif) 2014. Ref 17: Harcombe Z et al. Evidence from randomised controlled trials did not support the introduction of dietary fat guidelines in 1977 and 1983: a systematic review and meta-analysis. Open Heart 2015.
Ref 17: Harcombe Z et al. Evidence from randomised controlled trials did not support the introduction of dietary fat guidelines in 1977 and 1983: a systematic review and meta-analysis. Open Heart 2015.
Ref 18: Harcombe Z et al. Evidence from prospective cohort studies did not support the introduction of dietary fat guidelines in 1977 and 1983: a systematic review. Br J Sports Med 2016.
Ref 19: Harcombe Z, Baker JS, DiNicolantonio JJ, et al. Evidence from randomised controlled trials does not support current dietary fat guidelines: a systematic review and meta-analysis. Open Heart 2016.
Harcombe Z. Dietary fat guidelines have no evidence base: where next for public health nutritional advice? Br J Sports Med 2016.



I once irritated some people on Twitter by claiming that hypos were caused by too much insulin (or glucose-lowering medications) or booze because I couldn’t think of anything else. They were not the result of a carbohydrate deficiency. I believe the topic of discussion was type 1 diabetes (my brother), and a couple of type 1 moms were bursting at the seams, screaming, “If little Johnnie (whatever) doesn’t receive his snacks, fruit, nutritious whole grains, etc., he’ll have a hypo.”
Even for your high standards one of your best efforts. I enjoyed this as much as the JAMA article on cardiac risk factors for women. You didn’t just criticise the meat of the study, you also went for the conflict of interest of the advisors and the confirmation biases. This should be used to show medical students how to appraise papers, rather than just reading the conclusions. A few things that continue to annoy me in this world:
1 If you look for evidence of the benefits of low carb diets on the net, you will find papers from over a decade ago reluctantly conceding that they were superior, but then they trotted out the ‘lack of long term evidence’ caveat. Surely with all the research that is out there some of it must be long term by now?
2 There seems to be a wide spread consensus among low carb enthusiasts that ‘low carb’ starts somewhere around the 120 to 150 g per day, and that very low carb will be below that, for the sake of argument say under 30g per day. The point is that while the figures may be debated a bit, nobody I know that approves or are neutral about low carbs would ever say that 250 g per day was low carb, yet this would equate to 40% of a 2500 calorie diet and fit into the paper’s criteria.
3 The fact that low carbs could cause a hypoglycaemic attack is expressed as a bad thing, even though, as you say, the overall intention of diabetes treatment is to get the blood glucose down.When drugs (insulin and sulphonylureas) do it, it is a good thing, but if a diet does it it is bad. Cognitive dissonance again. Any doctor or diabetes specialist nurse knows that if a patient is consistently having hypos, the solution is to reduce the dose of the drug, or even cut it out completely. The confusion may arise in that during the acute attack you may have to give glucose to bring back normality, but it doesn’t mean that low carbs per se is bad – it’s the excess insulin that is ‘bad’ if we are going to use those terms.
4 Back to long term evidence again -David Unwin has shown that 46% percent of his selected group of type 2 diabetics on low carb diets still have diabetes reversed after 3 years, with normal weight and blood pressure and better lipid profiles, effectively reversing the metabolic syndrome. I would call NOT having the metabolic syndrome for 3 years, and still counting, a medium if not long term benefit, but I’m struggling to see where is the harm, unless it is the profit margins of the companies that make the drugs that they no longer are taking?
Hi Meddyg
You’re too kind!
I do remember starting to go through the consultation -as they asked us to – and thinking “hang on a sec…” And then approaching it as I wanted to.
It’s just such a fixed mindset – fat is bad, so carbs are good – and it seems quite immovable.
Yet – every person (diabetic or not) who wears a continuous glucose monitor – works out in a few days what is good for blood glucose and what isn’t. That’s what will lead us out of this madness I think! Patients will see through this.
Best wishes – Zoe
Funnily enough, the type 2 patients on insulin, spot fairly quickly that going on to insulin is not the answer to their prayers, because that is when they really start to pile the weight on. Well meaning diabetes nurses, as well as a lot of doctors think that all you have to do to correct the rising blood sugars that inevitably happen as insulin resistance worsens is to increase the insulin, but of course this is putting out a fire with petrol. Eventually insulin resistance is followed by patient resistance, as they realise that more insulin means getting fatter, and they sometime refuse to increase the dose. If you start trying to cut carbs at this late stage, you risk losing patient trust if they have hypos, especially if they end up in hospital, which is why it is far preferable to instill the low carbs idea at the very start. I appreciate that David Unwin has been very successful even for patients on mega doses of insulin, but hypo fear, which is what low carb critics use, is a very potent weapon for them.
Hi Meddyg
I upset some people on twitter once (ha ha – probably a lot more than once) by saying hypos were the result of too much insulin (or glucose lowering meds) or alcohol and I couldn’t think of anything else. They were absolutely NOT the result of too little carbohydrate. I seem to remember the debate was about type 1s (my brother) and a couple of mums of type 1s were exploding saying “if little johnnie (whatever) doesn’t get his snacks, fruit, healthy wholegrains etc he’ll have a hypo.” Yes – because you’re giving him too much insulin even for the insane amount of carbohydrate you’re giving him. Read the Bernstein bible, follow it and you’re type 1 might live a healthy long life.
Best wishes – Zoe
Thanks for this. Having listened to Tucker Goodrich expounding on the dangers of omega-6 Linoleic acid I suspect the authorities have chosen carbohydrates as the lesser of the evils – you can easily blame T2 diabetes on personal gluttony and sloth, cancer and AMD are probably harder to explain away, and the industries are well aware of the connections with seed oils in research going back 30 years. What are the food police expected to tell us to eat if protein is limited to 20% by common consent?
Cheers,
Pete
Hi Pete
Yes – Tucker – and Toxic Oils by David Gillespie and Nina Teicholz’s work – some great work has been done in this area.
If only animal fats were OK, all would be solved eh?! ;-)
Best wishes – Zoe