
Coronavirus – COVID-19 – some facts & figures

I’ve been writing a Monday note since 2009. The topic has usually been inspired by what’s in the news from a diet or health perspective. Whether the EAT Lancet diet being launched on the world, or the latest epidemiological paper to come out of Harvard – the topic that has made the headlines has been the one most likely to be featured.
This week there is only one health news story and it’s the same story worldwide – Coronavirus. I’ve been reticent to write about it, as the situation is uncertain and continuous, and this note will date faster than any I have written. (Hence why it’s coming out early – to be as current as possible). But it is the topic of most interest and so l will approach this topic as I would any other – What are the facts? What does the data tell us? Where best to find more information? I found the note very interesting to research and I hope you find it interesting to read…
What is Coronavirus? (Ref 1)
Coronaviruses (CoV) are a family of viruses that are called “zoonotic”, meaning that they are transmitted between animals and people. The word Corona in Latin means crown or garland. They are called coronaviruses because each virus particle looks like it is surrounded by a crown/garland when viewed under a microscope. There are four main sub-groupings of coronaviruses, known as alpha, beta, gamma, and delta.
Human coronaviruses were first identified in the mid-1960s. The seven coronaviruses that can infect people are split into ones that people commonly get around the world, but that have mild symptoms:
– 229E (alpha coronavirus)
– NL63 (alpha coronavirus)
– OC43 (beta coronavirus)
– HKU1 (beta coronavirus)
and three others, which have proved more serious:
– MERS-CoV (the beta coronavirus that causes Middle East Respiratory Syndrome, or MERS)
– SARS-CoV (the beta coronavirus that causes severe acute respiratory syndrome, or SARS)
– SARS-CoV-2 (the novel coronavirus that causes coronavirus disease 2019, or COVID-19)
When we are talking about ‘the coronavirus’ today, we are talking about COVID-19. This is a new coronavirus, which has not previously been identified in humans. We are dealing with something quite unknown with COVID-19, but we can learn some lessons from MERS-CoV and SARS-CoV. A paper published in the European Journal of Immunology on February 27th called “COVID-19: Lessons from SARS and MERS” is a valuable resource for anyone interested in understanding how the viruses are similar and different (Ref 2).
SARS-CoV originated in China in 2002 and ‘burned out’ in the summer of 2003 with the high temperature and humidity of the summer months helping to kill the virus. There have been no known cases of SARS anywhere in the world since 2004 (Ref 3). MERS-CoV was first identified in the Middle East in 2012. There is evidence that it is transmitted from camels, although transmission to humans is rare. There have been just five cases of MERS in the UK since 2012 (Ref 4). Neither virus has a vaccine, but it is likely that interest in developing one fizzled out alongside the numbers of people affected.
How did COVID-19 start?
The South Morning China Post reported that a 55-year old individual from Hubei province in China may have been the first person to have contracted COVID-19 on November 17th, 2019 (Ref 5). An academic paper published in The Lancet on January 24th 2020 reported on a cluster of pneumonia cases in Wuhan, China, caused by a novel coronavirus, which had been named 2019-nCoV (Ref 6). The article had undertaken a search to see if any other papers had been published about this new virus. It reported “No published work about the human infection caused by the 2019 novel coronavirus (2019-nCoV) could be identified.” This, therefore, appears to be the first academic paper about the virus.
This seminal Lancet paper reported that, by January 2nd, 2020, 41 patients had been confirmed to have what they called 2019-n-CoV (now called COVID-19). Of these 41 patients, 27 had had exposure to Huanan seafood market. The first patient of the 41 – identified on December 1st, 2019 – had not been to that seafood market. The common symptoms were fever (40 out of 41 patients), cough (31 out of 41) and fatigue (18 out of 41).
This paper reported that the Middle East Respiratory Syndrome coronavirus (MERS-CoV) and the Severe Acute Respiratory Syndrome coronavirus (SARS-CoV) had resulted in approximately 10,000 cases between the 2 viruses in the past 2 decades. The mortality rates were reported as 10% for SARS-CoV (Ref 7) and 37% for MERS-CoV (Ref 8), so we should be thankful that the case numbers were relatively small.
The first two cases of COVID-19 were reported in the US on January 14th, 2020 (Ref 9). The first case was reported in Australia on January 25th (Ref 10). The first two cases were reported in Italy on January 30th (Ref 11). The first two cases were reported in England on January 31st, 2020 (Ref 12).
What are the symptoms?
Common symptoms of having a coronavirus included fever, cough, shortness of breath and breathing difficulty. A British politician, Nadine Dorries, and a General Practitioner (Family Doctor) and former chair of the Royal College of General Practitioners, Clare Gerada, have recently recovered from COVID-19 in the UK and they have shared their experiences. Nadine is 62 years old and Clare is 60; both are fit and healthy women.
Nadine said that she started feeling “slightly unwell” and soon was experiencing fever, night sweats (to the point of soaking the sheets), sore eyes, a persistent cough (which was dry and unproductive) and every muscle and bone ached. She has been left with a residual cough and the feeling that her lungs have not yet fully recovered (Ref 13).
Clare returned from a conference in New York feeling like she had jet lag. This was soon followed by a temperature of above 102’f (38.9’c) and Clare realised that she had the virus. She spent the next five days in bed with flu-like symptoms – fever, dry cough, sore throat, bad headache, muscular chest pain from coughing (Ref 14). Clare reported a marked loss of appetite and I have seen this reiterated in other accounts from people who have recovered from the virus.
Chris Gough, an Anaesthetist, has had over half a million likes and retweets of his twitter thread detailing what he went through when he got the virus (Ref 15). I found this thread worth bookmarking because Chris detailed what happened on day 1, day 2 etc. Response to the virus will be individual, but this may be useful to look at if you develop symptoms.
The three key symptoms of COVID-19 are reported as fever, cough and shortness of breath (Ref 16). We understand that these can occur between 2-14 days after exposure, based on what has been observed with the MERS Co-V viruses. Most people will feel like they’ve got a particularly nasty dose of flu – for approximately seven days – and then recover. The minority of people – especially those with existing heart disease, respiratory disease, diabetes, hypertension, and/or cancer – develop more serious breathing difficulties and those are the ones advised to contact the emergency services.
Where can I get the latest information and data?
Many more academic papers have been published since that Lancet article. The academic database, PubMed, can be searched for “COVID-19” and “humans.” I did this and there were 99 results at the time of researching for this note (Ref 17). Papers range from individual case studies… to doctor experiences being shared to help other medics… to review articles about the virus particularly, or epidemics/pandemics generally. There’s even a paper about anti-Chinese sentiment during the outbreak.
The official information sites are the World Health Organization (WHO) (Ref 18), the CDC (US) (Ref 19), the NHS (UK) (Ref 20) and the Department of Health in Australia (Ref 21). Search engine companies have been working to ensure that the official advice is at the top of any searches that you do in your country.
The best real time data seems to be coming from Worldometers (Ref 22). This has more data, more up to date data and more different ‘cuts’ of the data than the WHO “situation” page (Ref 23). Worldometers is run by an international and independent team of developers, researchers, and volunteers. The team’s aim is “to make world statistics available in a thought-provoking and time relevant format to a wide audience around the world.” Their Coronavirus section provides the latest numbers of cases, deaths and recoveries per country (Ref 24). The data are also provided for men vs women, younger vs older people and people with different pre-existing conditions vs without.
What are the numbers?
The single most important thing to say about the numbers is that they’re wrong. There are two particular ways in which they are wrong, and we need to be aware of these, so that we don’t scare people unnecessarily:
1) Deaths will be the most accurate number, as official records are kept on deaths. The number of cases is the inaccurate number. We have not been testing anywhere near enough people and therefore the number of cases will be substantially underestimated.
2) The people most likely to have been tested are those who have symptoms of the virus. This is a form of confirmation bias. It will pick up more cases than there are in the general population, but it will miss the mild cases among the general population and thus again underestimate the number of cases and overestimate the severity of cases.
Both (1) and (2) will have the effect of making the death rate (deaths/number of cases) look worse than it really is (Ref 25).
The numbers are also changing every few minutes, so the following precise numbers will be out of date by the time you see them. They do, however, give a guide to the countries and types of people facing the greatest challenges and so are useful for trends and knowledge.
When I started writing this note, on 17th March, there were 189,000 cases worldwide, over 80,000 of which were recorded in China (42%). China did have all the cases (100%) in the beginning of this virus. China’s proportion of the cases is falling by the day, as case numbers rise in other countries. On the 17th March, Italy had the second highest number of cases in the world, followed by Iran, then Spain and then South Korea.
I updated the numbers at 7am on Friday 20th March and South Korea had fallen out of the top five. Italy has just overtaken China for the number of deaths. I’ve kept S Korea in the following table, as its testing numbers are interesting. China’s proportion of cases has dropped to 33% in 3 days.
The table below is a snapshot of the top five countries, plus S Korea. This illustrates available data. You can get the latest numbers from the Worldometers site and/or for your own country, as desired.

The table extracts data for: cases, deaths, cases per 1 million people in that country, tests per 1 million people (these data are not available for most countries and the two numbers above were from March 9th, 2020) and the population of each country. I have also calculated deaths per number of cases. This is NOT an accurate picture of the death rate, as I started to explain above and continue here…
As you can see from the table, testing has been very low, and we don’t even know the testing rate in most countries. The key message from the WHO conference on March 16th, 2020 was “test, test, test” (Ref 26). We don’t know what we’re dealing with without facts. Testing has been grossly insufficient worldwide since this virus started. Don’t think, from the table above, that S Korea has a death rate of 1.1% and Italy has a death rate of 8.3%. Italy has tested a quarter of the number of people that S Korea has. It may be the case that half the Italian population has the virus, and thought they had flu, in which case the death rate would be 0.007% – you won’t be able to get your head around such a small number.
A tweet on March 13th questioned: “Can anyone explain how a virus (identified in Wuhan in Dec 2019) spread to the Canadian prime minister’s wife, one of Hollywood’s top actors & his wife, a Premier League football manager, and a British member of parliament – within 16 weeks – while bypassing the majority of us?” (Ref 27). The answer is, of course, it didn’t. Many of us have, or have had, the virus already.
The high risk groups
The data on Worldometers can be cut by sex, age and existing conditions. This is where the numbers can appear scary, but keep in mind that we are underestimating case numbers. The three messages that we get from demographics are:
1) Sex: Worldometers calculates the deaths/cases to be 2.8% for men and 1.7% for women. Smoking is a risk factor for respiratory diseases; most of the deaths have been in China (until this morning) and 52% of men smoke in China vs 2.7% of women (although women are exposed to second-hand smoke) (Ref 28). If you’re male and don’t smoke, this should reassure you. If you are a smoker of either sex, it is recommended to do whatever you can to quit now. Smoking up to the point of contracting the virus won’t help chances of recovery.
2) Age: Worldometers calculates the deaths/cases to be as follows per age group:

Italy is the country to mention in the age category. There are a number of different ways of calculating the age of a population. Italy has the third oldest population in the world when calculated by people over 65 per working age people (Ref 29). An article on Italy was shared by a Swedish American academic in an email thread (Ref 30). People who have died in Italy had an average age of over 80, were predominantly male (think smoking again) and had an average of 2.7 pre-existing health conditions (Ref 31).
We all have older loved ones and the numbers for older people have been the most worrying but i) keep remembering that this number is higher than the truth and ii) pre-existing conditions overlap significantly with age. Older people are more likely to have other conditions (see the next section).
3) Pre-existing conditions: Worldometers calculates the deaths/cases to be as follows per pre-existing condition:
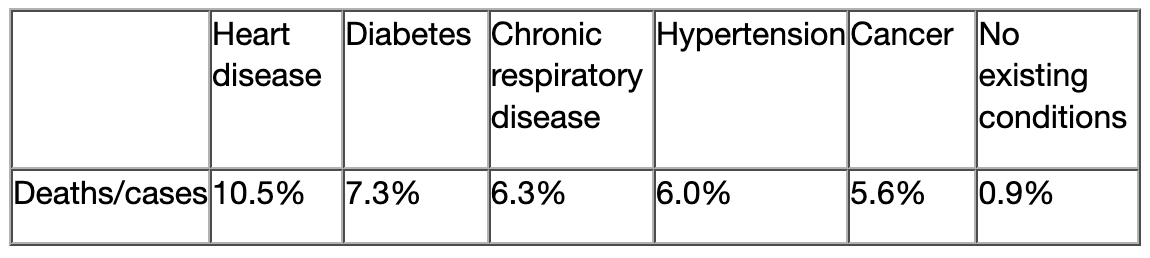
The 0.9% deaths/cases for “no existing conditions” cuts across all ages, so the reassurance for healthy older people should come from this existing condition data. The current strategy to protect older people and those with existing conditions should perhaps focus more on the latter than the former, but caution is wise for all higher risk groups when facing unknowns.
Reassuring numbers
There are enough scary numbers being shared at the moment. Here are three that reassure me:
1) The number of active cases has peaked and is on the decline in the country that first experienced the virus. (This does provide support for China’s response to the virus).

2) I have added a calculation into the table for the top five countries (plus S Korea) to put the number of deaths in perspective. Every death is a loved one lost. This is not to diminish the suffering that is being felt in any way. It is to provide perspective because perspective can ease fear and fear is as big an enemy as the virus right now:

3) Pollution kills an estimated seven million people worldwide each year. A number of deaths will have been avoided because economies have been operating far from normally (Ref 33).
Closing thought
Current deaths worldwide stand at 10,049. The flu claims approximately 400,000 lives every year, the majority of which – as with COVID-19 – are among the elderly and the vulnerable (Ref 34). We don’t close down nations and panic buy toilet rolls because of the flu.
There’s a lot of ‘scaring the life out of people’ going on right now – in print and online media and on social media. It isn’t helpful. Caution yes, catastrophising no. I hope that we will look back on this time and see that the above table was reflective of the outcome and COVID-19 barely made it onto the list of major causes of death for any country.
In the meantime, we need to be the best people we can be. The ones helping the vulnerable, not hoarding provisions for ourselves. I will always fear what humans can do to each other more than what any virus can do to ourselves.
References
Ref 1: https://www.who.int/health-topics/coronavirus and https://www.cdc.gov/coronavirus/types.html
Ref 2: Park et al. COVID‐19: Lessons from SARS and MERS. European Journal of Immunology. 27 Feb 2020. https://onlinelibrary.wiley.com/doi/10.1002/eji.202070035
Ref 3: https://www.nhs.uk/conditions/sars/
Ref 4: https://www.nhs.uk/conditions/middle-east-respiratory-syndrome-mers/
Ref 5: https://www.scmp.com/news/china/society/article/3074991/coronavirus-chinas-first-confirmed-covid-19-case-traced-back
Ref 6: Huang et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. The Lancet. January 24th 2020 https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)30183-5/fulltext
Ref 7: https://www.who.int/csr/sars/country/table2004_04_21/en/
Ref 8: https://www.who.int/emergencies/mers-cov/en/
Ref 9: https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/cases-in-us.html
Ref 10: https://www.health.gov.au/news/information-about-the-first-confirmed-case-of-novel-coronavirus-in-australia
Ref 11: https://www.epicentro.iss.it/coronavirus/aggiornamenti
Ref 12: See 31st January update https://www.publichealth.hscni.net/news/covid-19-coronavirus
https://www.publichealth.hscni.net/sites/default/files/2020-02/COVID-19%20-%2031%20January%202020.pdf
Ref 13: The Sunday Times 15th March 2020. https://www.thetimes.co.uk/article/nadine-dorries-the-doctor-broke-the-news-i-had-the-coronavirus-and-i-gave-it-to-mum-hkx2hjpbd
Ref 14: http://www.pulsetoday.co.uk/views/blogs/as-a-gp-whos-overcome-coronavirus-heres-what-i-want-you-to-know/20040354.article
Ref 15: https://twitter.com/GoughCJ/status/1239587299136098305
Ref 16: https://www.cdc.gov/coronavirus/2019-ncov/symptoms-testing/symptoms.html
Ref 17: https://www.ncbi.nlm.nih.gov/pubmed/?term=covid+19
Ref 18: https://www.who.int/health-topics/coronavirus
Ref 19: https://www.cdc.gov/coronavirus/types.html
Ref 20: https://www.nhs.uk/conditions/coronavirus-covid-19/ and https://www.gov.uk/guidance/coronavirus-covid-19-information-for-the-public
Ref 21: https://www.health.gov.au/news/health-alerts/novel-coronavirus-2019-ncov-health-alert
Ref 22: https://www.worldometers.info/about/
Ref 23: https://experience.arcgis.com/experience/685d0ace521648f8a5beeeee1b9125cd
Ref 24: https://www.worldometers.info/coronavirus/
Ref 25: The top number (the numerator) will be accurate and the bottom number (the denominator) will be lower than it should be. This means that the rate – the top number divided by the bottom number – will be higher than the truth.
Ref 26: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19—16-march-2020
Ref 27: https://twitter.com/DavidVidecette/status/1238487118030258180
Ref 28: Parascandola & Xiao. Tobacco and the lung cancer epidemic in China. Transl Lung Cancer Res. 2019 May. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6546632/
Ref 29: https://www.weforum.org/agenda/2020/02/ageing-global-population/
Ref 30: https://www.thelocal.it/20200311/coronavirus-what-do-we-know-about-the-victims-in-italy
Ref 31: https://www.iss.it/en/comunicati-stampa/-/asset_publisher/fjTKmjJgSgdK/content/id/5304852
Ref 32: https://www.macrotrends.net/countries/CHN/china/death-rate (and then other countries can be searched)
Ref 33: https://www.who.int/health-topics/air-pollution#tab=tab_1
Ref 34: Paget et al. Global mortality associated with seasonal influenza epidemics: New burden estimates and predictors from the GLaMOR Project. J Glob Health. 2019 Dec. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6815659/


Aren’t we underestimating the risk of having underlying illness? 48% of American adults have cardiovascular disease. The CFR (Case Rate Fatality) for those with CVD and COVID-19 is 10.5%. 55%-59% of Italian adults have hypertension. The CFR for those with hypertension and COVID-19 is 6%. Could a high proportion of underlying illnesses be the reason we see countries such as Italy overwhelm their healthcare system? Also, flu cases and deaths are estimated. We have concrete data for COVID-19 (though yes, the # cases is likely inaccurate). It appears that COVID-19 is much more contagious than influenza, which means if a higher proportion of an unhealthy population gets it, the higher the deaths.
Excellent article but weak on China. No way that Chinese utterings are remotely true. Deaths will be much much higher. They cannot be remotely believed that there are no new cases and that death rate is falling.
During the winter months (flu season) my partner and I take extra vitamin C, Vitamin D3 and quercetin. I’m hearing now that this is being adopted throughout many progressive hospitals and this has greatly reduced the mortality rate. I do understand that high dose vitamin c is given intravenously immediately on admission and I believe that they are doing the same with vitamin D. The UK does not appear to be using these tactics. Information coming from China indicates that they are using up to 12000 mg of vitamin C but the usual ratio seems to be 6000 mg of vitamin C, 1500 IU of vitamin D and 1000 to 1500 mg of quercetin per day.
This article is extremely informative and well written for the most part – with the exception that you have only looked at the death rate.
The death rate is not the only vital piece of information, the hospitalisation rate is equally, if not more important.
Young and healthy people are also becoming hospitalised. While the hospitals can keep up, this is not such a problem. If the hospitals become overrun, more people start to die. The death rate in China has dropped due to very stringent (harsh) quarantine methods. Now it is starting to level out in Italy because of quarantine measures too.
This is not “just the flu”
Thanks for the research.. I’l be forwarding your link and references to the national team where I’m living
a slightly different Take away..
[ from my recent post at.. .facebook.com/charles.laws.1610 ]
” Covid-19 ! is what seem to have taken hold of just about every one! So I’d like to look at the numbers that I gleaned from various nespapers and news media online My primary source was a detailed story of a Boston doctor and 5 friends who went to Miami on March 5th..and went their own ways on March 9th. and did not show or experience any “ïllnes” until several days later..
Testing was not undertaken for a couple more days, with positive results available several days later
Did the testing do anything for them? NO !
Did it do anything to reduce the spread of the virus -n this instance NO!
This evidence indicates that identifiation and treatment of the disease DID NOTHNG to prevent a pandemic… and the hysterical disruption of the global economic system following dramatic reporting of cases, numbers of those tested, of tests available , hospital beds required and deaths and all the attendant emotional reaction that have sent the world’s social systems into chaos are — > absurdities.
It MIGHT be stopped, before decimating the susceptible population, ONLY IF we understand that it becomes the responsibility of all of us -individually- to do whatever we can to not infect others. Self isolate.. by choosing -not to infect others.. because we might have been infected, and are still without any symptoms-
What’s the time required?
From the moment of possible exposure.(as direct transfers are possible by contact and even from a variety of possibly contaminated surfaces) to the times that have passed and demonstrated the virus to be inactive, or absent in all members of a closed commnity ..
An insurance co. actuarial calculation, or skilled statistician / mathematician could estimate the required time to reduce the viral presence to 0, -the extinction of the virus.. But I’m sure it is longer than 14 days ..or even the 19 imposed by Columbia’s lock down, or the de facto lock downs imposed by various countries closure of borders.. representing a form of -National self isolations- that do not comprehend that they probably already have the virus.(and it can continue to spread internally).
What’s best? Assume that you are infected and thus potentially responsible for the communication to others and the perpetuaton of the virus, pandemic and resulting global disruptions.. Take a secluded vacation, and a few weeks to clean the house and yard, watch a TV or movie, read a few books.. and find normalcy in a very limited social life..
AH !
a subsequent addition was
” Ha ! >> an additional note —SPREAD the message– NOT the DISEASE.! ! —
You say:
“Many of us have, or have had, the virus already.”
That changed my perspective!
Is it possible that I have?
And at 72 didn’t notice it?
(I wish I could check for anti-bodies, etc!).
Hi Barry
I was chatting with Andy at dinner about the bizarre collection of people who had shared that they had the virus and then that tweet just summed it up so well: “Can anyone explain how a virus (identified in Wuhan in Dec 2019) spread to the Canadian prime minister’s wife, one of Hollywood’s top actors & his wife, a Premier League football manager, and a British member of parliament – within 16 weeks – while bypassing the majority of us?”
It hasn’t bypassed us all, so some people have it and some people have recovered without even knowing they have had it. The latter would more likely be younger people who seem less affected. There’s lots on testing in the papers today and talk is about testing for those with antibodies as well as for those with the virus. Both can help to inform vaccine research. Plus – if any people have antibodies, they can be invaluable right now. Tests are in short supply of course. Health care workers should be prioritised and then those self isolating can know for sure if they need to stay away from others.
Given that the first UK case was 31st Jan, unless you’ve had a high fever and a persistent cough since then and felt pretty bad for a few days, you’re highly UNlikely to have had it. Stay safe!
Best wishes – Zoe
Thank you, Zoe, for this reasonable assessment of numbers. I’ve been thinking about subscribing for a while, but this article made up my mind. It amazes me how readily Americans are going along with a complete loss of civil freedoms and economic health in the goal of “not overwhelming hospitals.” Surely we could target our response to specifically protect the vulnerable and build hospital capacity while letting the 99% of low-risk individuals go about the business of living and building some actual herd immunity. The Italy story is especially irritating – why are we shocked that some 3400 octogenarians have died over a month? Why do we count the deaths of people at the end of their lifespans in this total? Italy is what everyone seems to cite – OMG, we don’t want to be like Italy! So sure, college students should happily toss away a semester, hourly workers should smile as they lose their incomes, we should give up any hope of planning for anything, and I should be delighted to be prevented from visiting my 72-year-old mother who lives alone but in another state. Insanity.
Sorry Aimazoid.. I think you are missing an essential point. i.e. The potential of transmission and multiplicaton of numbers that occurs prior to any symptoms are felt or observable.. plz ceck out my post @ facebook.com/charles.laws.1610
Hi Zoe, as always, what you’re best at is sifting the wheat from the chaff and getting nearer to the truth, although for now, we’re a long way from that.
Re symtoms, I just wanted to add that loss of smell (anosmia) is being increasingly reported, particularly in those under 40 without any other symptoms.
This statement gives more info. Important to know about this as it’s not one of the symtoms that trigger self-isolation in the UK but people should be aware of it and make their own decision
https://www.fifthsense.org.uk/covid-19-corona-virus-and-smell-loss-guidance-from-fifth-sense-medical-director/
Take care
Simon
Dr Simon Tobin FRCGP
I’ve been asking this continually and still cannot figure it out. Who benefits from destroying the WORLD’S economy? I just cannot figure it out, but I do not believe this is simply a reaction to a virus. I have never seen worldwide border closings for a virus that, admittedly most people can get, but that is deadly to the minority who get it. There’s absolutely no logic to it, so it has to be something else
An increase in confirmed cases is, at best, a poor proxy for the spread of the disease. Since the baseline of tests has been so low, the discovery of more confirmed cases only tells us that there has been more testing. Since confirmed cases are being treated as an absolute indicator of spread by media and gov’ts, the panic will increase as the testing increases. A temporary exponential increase in testing will be seen as exponential growth of the disease. My estimate is that on a log curve, as the number of confirmed cases gets to 8m, it will take too long to double again and the panic will subside.
The rulers of this planet want one economy i.e. one currency and they need it to be digital, so in order to implement that they they to take out the current system and replace it with the new world order. The ultimate goal is to install the insignia of the coming world ruler that one has to accept if you want to buy or sell anything (Rev. 13:16-19). Please take this seriously there’s much more to it than what meets the eye…/Andreas
Thank you! Finally, a voice of reason. I notice when facts like this are posted, inevitably the main counterargument are anecdotal and pathos based. The world economy is tanking because of this, and that could have far reaching consequences, including [indirectly] on health
There doesn’t seem to have been an increase in excess deaths in Europe this winter according to this site https://www.euromomo.eu/index.html
And this looks interesting: https://www.ncbi.nlm.nih.gov/pubmed/32133832?fbclid=IwAR1Qf8jFBYSec0w8ieuHjbVs8BMRaYrRwyJlZq-cRF5sEklz2H9QCNmy9DU
So that second link is saying that possibly at least half the people who are alleged or assumed to be infected, but asymptomatic, are clear?
My worry relates to avoidable deaths. At the peak of an outbreak of this novel virus, health systems struggle to have the intensive care capacity, leading to patients not getting the care they need, doctors having to make choices on who to save and who not to save, and a desperate time for all. Surely we must to everything we can to prevent the surge in cases reaching the level at which our ICU capacity ceases to cope. I certainly don’t want any of my loved ones to lose their lives avoidably because of insufficient capacity at the height in if this epidemic, so I think we all need to do everything we can to take action to reduce the peak of this outbreak. And whilst I do think people need to stay calm on toilet rolls, I absolutely think we need to take this outbreak very very seriously. This is not flu
Why worry relates to avoidable deaths. At the peak of an outbreak of this novel virus, health systems struggle to have the intensive care capacity, leading to patients not getting the care they need, doctors having to make choices on who to save and who not to save, and a desperate time for all. Surely we must to everything we can to prevent the surge in cases reaching the level at which our ICU capacity ceases to cope. I certainly don’t want any of my loved ones to lose their lives avoidably because of insufficient capacity at the height in if this epidemic, so I think we all need to do everything we can to take action to reduce the peak of this outbreak. And whilst I do think people need to stay calm on toilet rolls, I absolutely think we need to take this outbreak very very seriously. This is not flu.
Zoe, I found your article to be very well researched and well written. Thanks for a deeper insight into our latest common issue.
I usually very much respect your views Zoe, but have you actually seen the footage of Italian hospitals utterly overwhelmed by the numbers of critically ill patients? Of doctors and nurses pleading for help? I would like to be reassured but I think this needs to be taken seriously. I live in London. My daughter is recovering from Covid-19. She hasn’t been tested but had been in contact with someone (one of her students) who did test positive. Two of my son’s friends are recovering from it. I can assure you no-one would confuse this virus with a dose of seasonal flu. In the US 40% of those hospitalised are reported to be 20-54. Even if they don’t die, their health will be compromised. This is a new virus for which there is no treatment and no vaccine. It’s dangerous because, in some people, mainly the elderly and vulnerable, but not exclusively, the immune system is overwhelmed. One Italian doctor working in an Intensive Care ward in Northern Italy was very depressed because of the 140 patients who had been admitted to the ward with C-19 complications, not a single one had recovered. Not a single one! Please take care not to give false reassurance. This really is serious and it’s irresponsible of you not to treat it as such.
I totally agree. Whilst the numbers are misleading (and thank you Zoe for putting perspective on this), it’s the SEVERITY of this disease that’s frightening. It targets the lungs, both the ciliary and mucous cells, frightening.
The Drs and Nurses will never be the same again after this.
Your report leaves out what in my view drives government response to this crisis. Peculiar for Covid-19, unlike the flu, is the huge impact on hospitals, and in particular on ICU units. The large number of patients that need to be put on ventilators. This does not just require a bed, but ICU units operate on 1 nurse for each patient, 24/7. So, just do the math, you need a team of 4-6 skilled nurses to attend to 1 patient during a week. Now you look at the number of Covid patients flowing into ICU units, and you see hospitals collapsing. Happened in Northern Italy, is happening in south of the Netherlands right now, will happen in all of the Netherlands in 7-14 days. For NL you can watch daily ICU load in the website stichting- nice.nl, a foundation by and for ICU MD’s. You can watch the Italian style disaster taking shape in NL on the next week or two. Thus is driving government response, and in NL and UK also political conflict. Because if the government doesn’t stop the inflow to ICU units with drastic measures, the government will be blamed for the total collaps. Government will be blamed for death of patients who are refused ICU because there is no place for them, unless they take at least drastic action, if not timely.
“ICU units operate on 1 nurse for each patient”
Not sure where you are, but in the U.S. ICU patient to nurse ratios are often 2:1 (2 patients per 1 nurse in ICU) and many go 3:1, unless they are in California, which has mandated ratios (2:1).
What is the takeaway at focusing that the “Rate” is being reported to high, if the serious cases and deaths stay the same (just the total infected goals up). It still leads to the same issues we are seeing in Italy and NY now (and previously China).
The rate is not the important figure, the deaths and serious cases are, so recalcuting the rate may help people feel safer but doesnt impact the true issue. Hospitals face being overrun with more supplies, which will lead to high number of deaths.
Zoe, you are the voice of reason, as per usual. Thank you for another excellent article.
I want to know the reason for all the hype. Someone somewhere has an agenda and the media and governments are playing along. I can see that Big Pharma stands to make a fortune peddling its vaccines but why wreck the economy unless it is to ensure that everyone is forced to have their vaccine regardless “just to make sure that we don’t get this again”. Even that doesn’t make sense because those who have had the virus will have lifelong immunity. I think that we should all go out and hug each other then we won’t need Big Pharma’s rubbish.
It’s obvious China’s numbers are made up. They are lying about their stats and not recognizing any new cases.
The Italian health agencies are reporting escalating COV19 deaths—big fear-story out front…
But in the background, other Italian government researchers are combing through patient records, to take a much closer look…to see whether people are dying from the virus or other more obvious causes.
Are people dying coincidentally WITH the virus, or BECAUSE OF the virus? Is the virus a mere harmless passenger in the body, or is it the driving force? The Italian results are astonishing, to understate it by a mile.
Bloomberg News has the story: 3/18, “99 percent of those whose died from virus had other illness, Italy says”: “More than 99% [!] of Italy’s coronavirus fatalities were people who suffered from previous medical conditions, according to a study by the country’s national health authority.”
“The Rome-based institute has examined medical records of about 18% of the country’s coronavirus fatalities [so far, because it’s slow work], finding that just three victims [!!], or 0.8% of the total, had no previous pathology [disease]. Almost half of the victims suffered from at least three prior illnesses and about a fourth had either one or two previous conditions.”
“More than 75% had high blood pressure, about 35% had diabetes and a third suffered from heart disease.” “The average age of those who’ve died from the virus in Italy is 79.5 [!!!]. As of March 17, 17 people under 50 had died from the disease. All of Italy’s victims under 40 have been males with serious existing medical conditions.”
Lots of prior medical conditions, weakened immune systems, and what this emerging study isn’t saying: all these people had obviously been treated for those prior conditions with (no doubt site effect riven) medical drugs. Furthermore, once they’d been diagnosed with coronavirus, chances are many of them were put on highly toxic antiviral drugs. Thus delivering the final blow or Coup de grâce.
Imagining the coronavirus was the CAUSE of death would be a ridiculous fantasy. But these people are counted as “coronavirus deaths” by the other Italian reporting agencies, who are jacking up the numbers.
The elderly people with obvious prior diseases who died in Australia; and the elderly people who were diagnosed as coronavirus cases in the state of Washington—all living in a long-term-care nursing home?
This death-numbers con—aside from covering up the real causes of death, including MEDICAL—is the forward spear being used to justify locking down and wrecking economies all over the world right now, and that means attacking the people in any way connected to those economies who have to work to make a living.
Just because people have a “previous medical condition”, doesnt mean you were expect to die or that you can attribute your death to that. Most of the world’s population has a “previous medical condition” whether is asthma, obesity, diabetes, high blood pressure. Your essentially saying to discount all deaths outside a perfectly healthy 18.
“So what you are say is”…….NO but when this insanity finally comes to an end see what the figures really are. How ever because the “experts” are saying the Emperor has nice new cloths do not expect this to happen over night.
The problem is that there a) isn’t a vaccine and b) our health service, as seen in Italy, cannot cope.
Can’t take issue with any of Dr. Harcome’s conclusions except to point out that we are still in the early stages of this pandemic. She is right in that the “confirmation bias” introduced by the unknown number of infections, (those with few or no symptoms), biases the death rate upward. It’s basic math. The actual infected denominator is probably much higher. 2. Lacking accurate and comprehensive test data is making adequate assessments of corrective measures very difficult. 3. The hospitalization rate for this virus as it peaks in the population appears to be much higher (20%) which has the potential to over-run our hospital capacity. So, lacking a vaccine and lacking accurate infection information social distancing is the best tool available until those realities change.
Hi Zoe, thank you very much for this article which has allayed any fears I had. I have a daughter who has had to come back to Wales from Switzerland because her resort closed. She is young and constantly reads social media and was frightening the life out of me ! I naturally have a very laid back attitude to all this but am cautious because I look after my mother who is 98 and still going strong. She by the way is not phased by any of this having being a child when infections could just take you off and of course the war in London.
I too am more worried by what humans can do to each other more than viruses or apoliptic zombies.
Thank you again and take care.
Christine
Hi Zoe,
Love your work and agree with everything you’ve laid out here. Could you please comment on the issue of lack of health care system capacity to care for the large influx of patients with severe disease all at once if measures are not taken to slow the spread, and how that might influence the death rates? This is not a big issue with flu because cases of of flu are spread out over the course of several months each year. In general, people who die from the flu do so because they are very sick, not for lack of ventilator availability or health care resources. COVID19 is different in that it is novel and spreading rapidly, so the potential to overwhelm healthcare systems as is happening in Italy all over the world is a very real threat and would result in not only many more lives lost but also the collapse of health care systems to provide care that is still needed for many people. Thanks Julie
Hi Julie
This is a really good point. The capacity does appear to be an issue – the issue? – in Italy if not elsewhere.
This is also where the panic is not helping because people are turning up at ICUs who would not previously have thought of going there. With flu, given the number of deaths, it would appear that an elderly relative feels unwell, takes to their bed and then the family is devastated when they don’t recover from this. But they rarely go to the ICU – maybe they should. This virus will certainly teach us things when we are able to look back with more knowledge than we have now.
(What this also means is that far fewer people come into contact with people who have the flu – because it comes on so suddenly and people just take to their beds and most recover without seeing other people. COVID-19 is around for that 2-14 day period without necessarily showing symptoms and that’s when it is most likely to be passed on.)
The UK Chief Medical Officer, in a recent update press conference, said “Over 44,000 people have already been tested, of which over 42,000 were negative.” Those were people who turned up at a medical centre – not necessarily an ICU – but a medical centre and were tested for the virus. 42,000 of those people effectively turned up and didn’t need to. We can all understand why they did. I think everyone in the affected countries right now wants a test – have I had it already? do I have it? etc
People who feel unwell now are understandably scared and want the best medical attention possible. More people want tests, more people want care. We have had hospitals in the UK declare emergencies over the past few winters when people have come in with flu and their capacity has been reached. This is the same kind of demand, but amplified.
For me it just keeps coming back to don’t panic. Panic won’t help. Panic will make things worse. We need calm heads. I have 5 high risk close family members and I’ll be doing everything I can to keep them out of hospital – not least because I’m not sure that’s the best place to be for most people right now.
Take care
Best wishes – Zoe
Thanks for your response and I completely agree – panic is not helpful! We need to just make the best decisions with the info we have now (which is not a lot) and press for better data so we can make better and more informed decisions as the weeks go on. Thinking of you, Andy and your family and hoping you all stay well and healthy! Julie
50% or so of the Covid-19 people are asymptomatic carriers. This has been shown in Vo, Italy and Iceland. This means they (supposedly, the theory is) give the virus to others while being oblivious themselves.
Patient 31 in South Korea supposedly caused the infection of over 1,000 people.
https://graphics.reuters.com/CHINA-HEALTH-SOUTHKOREA-CLUSTERS/0100B5G33SB/index.html
Also, the people who go to the hospital stay in the ICU for about a week with covid-19. This includes both those who recover and those who die. One week. When you have limited beds and ventilators, this is bad.
Where I live (Connecticut, USA), it’s so bad our local hospital is already full according to the governor. (Though I’ve seen elsewhere that they still have some capacity.) And because we can’t test, 200 nurses there who came in contact with Covid-19 patients have been sent home. They can return if we can test them and prove they do not have covid-19.
Our response in the US has been abysmal. We got a positive test the same time South Korea did. But they went on a campaign of testing many people. Their infection rate is decreasing because of testing and isolation. We STILL can’t test the people we need to test.
Moreover, our president told the governors of our states to go find their own PPEs (Personal Protective Equipment). Think about that. Because our president hates the government and we don’t have a coordinated response from the federal gov’t, you now have 50 governors who have to find where these things are made and make deals with the manufacturers. What if the output is limited and say only 20 states can get PPEs? Is there a bidding war? Do certain states simply not get them? If you’re a governor of a state with a manufacturing facility, do you take all the PPEs and not let anyone else have them? We need some federal government oversight and help (that’s why we HAVE a federal government), and we aren’t getting anything. I
Just take a look at the rate in NYC. It’s exploding, partly because of testing. It’s doubling daily, at least recently. Even if only a small percentage of those are critical and have to go to the hospital, that will overwhelm the hospitals, especially if they stay in the hospital over a week each. Compare that with the flu — I’ve personally never heard of anyone being in the hospital for the flu, let alone being in the ICU for 1 week. Moreover, the disease lasts about three weeks if you get, at least that’s the data I find. Both my daughters got the flu this year (first time ever), and they were completely recovered in a few days.
Where you are, it might not get bad. But I think the US got way behind in this and I think some medical systems will be overwhelmed, similar to what happened in Italy.
“Compare that with the flu — I’ve personally never heard of anyone being in the hospital for the flu, let alone being in the ICU for 1 week. ”
You must not work in a hospital during flu season. Approximately 5-10% of hospital admissions for flu are admitted to ICUs (https://www.ncbi.nlm.nih.gov/pubmed/30481669).
“In 2004, there were over 37,000 hospitalizations in which influenza was noted during the hospital stay, and more than 21,100 hospital admissions resulted principally from influenza—a 62 percent decrease from 2003, but twice the number of hospitalizations in 2001.” (https://www.ncbi.nlm.nih.gov/books/NBK63484/)
‘The in-hospital death rate for patients 85 years and older with influenza was more than twice the in-hospital death rate for influenza patients between 65 and 84 years of age (7.9 percent versus 3.3 percent).” (https://www.ncbi.nlm.nih.gov/books/NBK63484/)
The reason you “never heard” of it is because it’s not newsworthy, and the flu season is a “season” lasting from around October to April/May (https://www.cdc.gov/flu/about/season/flu-season.htm), so most hospitals are able to, mostly, deal with the increase in patient admissions. It’s been a part of hospital life for a long time and the system has adapted to it. And don’t forget that there is a vaccine (maybe not perfect) that may have a factor in lessening the impact.
Covid-19 is like having the entire flu season in one week. And it’s the ONLY thing being talked about. A rapid influx of a NEW respiratory viral illness during the FLU SEASON is not what any hospital needs. That’s why you’re no longer hearing about the flu, or about anyone being admitted to an ICU for it, but trust me, it’s still happening.
Thanks for writing this Zoe, you’re level-headedness is a relief. Wish you were on the news. I especially like your chart of virus deaths vs. “normal death rate.” It is so important to remember that, sadly, people are always dying.
I had a slight temperature and a bad cough a couple of weeks ago – it might have been coronavirus or it might not. I did not experience shortness of breath. However, until recently I was severely asthmatic so I know what shortness of breath feels like. I tried going paleo for a while with a boiled egg for breakfast and the asthma cleared up. But a boiled egg is a depressing way to start the day. So I went back to porridge, but made sure to soak it overnight in warm water mixed with whey so that the oats would ferment slightly. No more asthma. If I eat unsoaked porridge the asthma comes back. I think my problem was inflammation of the airways. I would suggest that anyone experiencing shortness of breath should try dietary changes in the direction of high fat low carb to reduce inflammation. And eat slightly fermented porridge.
Try frying an egg, scrambled or an egg as a cheese omelet, coddle an egg, or bake an egg. Recipes abound! Eggs aren’t depressing – they are nature’s perfect food! Add some bacon for LCHF. Porridge is not LCHF because it is made from a grain aka very High Carb, indeed…even when slightly fermented.