
LCHF & butter
I was interviewed for a couple of podcasts last week and the interviewers, the “Keto Dudes”, were particularly interested in the PURE study (Ref 1). I wrote a post on that last August (Ref 2). One of the most interesting findings from the PURE study was that it gave us global empirical evidence for protein intake across many different diets in 18 countries and 5 continents. The podcasts also covered the work I’ve done on dietary fat guidelines. Then a thread in our club about butter got lively. Putting the three themes together has made for an interesting, possibly controversial, Monday note…
When I submitted this paper (Ref 3) for peer review, one of the comments that came back was “what’s the reference for the claim that protein is approximately 15% of natural diets?” It was a good point. The answer “it just is!” (because I have analysed so many diets and seen the constancy of 15% each time) rightly wasn’t going to appease the reviewer. I thus added the Gordon/Wardlaw nutrition ‘bible’ reference, which gives examples of typical daily diets showing that protein tends to be close to 15% in the different examples (Ref 4). The PURE study confirmed the small variation in protein intake in a wide range of diets. Five of the seven regions, covering 75% of 135,000 study participants, had protein intakes of between 15-17.5% of energy intake. Africa and south Asia had slightly lower protein intake: 13.4% and 11.6% respectively.
Macro nutrients
There are three macro nutrients. We know them as carbohydrates, fat and protein. These are the parts of food that deliver energy, which we measure in units called calories.
In 1977 in the US, and in 1983 in the UK, dietary fat guidelines were introduced. The two key guidelines were that we should consume no more than 30% of our daily calorie intake in the form of total fat and no more than 10% in the form of saturated fat (Ref 5). The important corollary, with protein staying fairly constant, is that setting a total dietary fat guideline of 30% means that a carbohydrate guideline of 55% has inevitably also been set. For the avoidance of doubt, the 1977 report “Dietary Goals for the United States”, spelled out the implication of the fat guideline: “Increase carbohydrate consumption to account for 55 to 60% of calorie intake” (Ref 6).
Current Dietary Guidelines
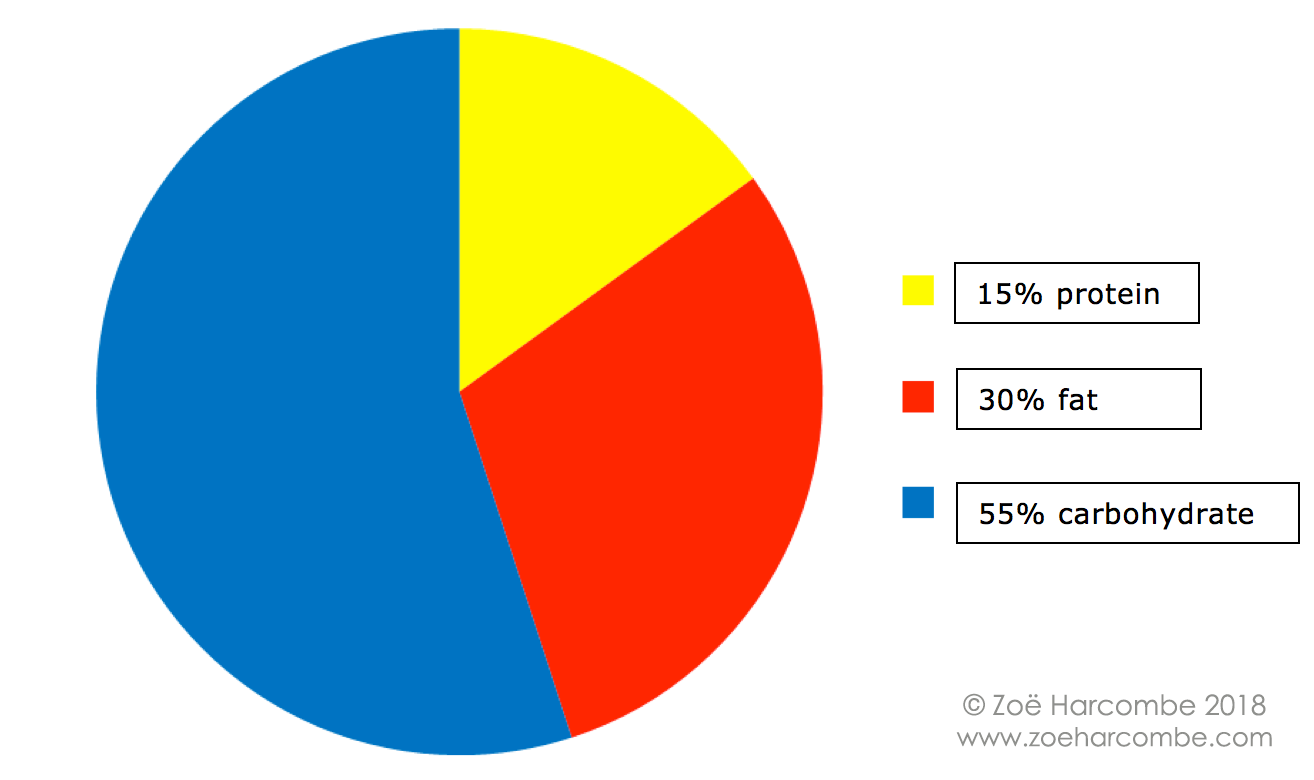
The constancy of protein means that setting a fat maximum creates a carb minimum and, equally, setting a carb maximum sets a fat minimum. However, this doesn’t mean that we should do unhealthy/unhelpful things for the sake of it – just to achieve certain macronutrient ratios. We can drive the proportion of fat in our diet even lower by eating more carbohydrate. Equally, we can drive the proportion of carbohydrate in our diet even lower by eating more fat. Are these good ideas ‘for the sake of some ratios’?
LCHF
If protein remains approximately 15%, choosing to set a carbohydrate upper limit of 5% of daily intake implies that the remaining 80% will be consumed in the form of fat – as shown in the pie chart below:
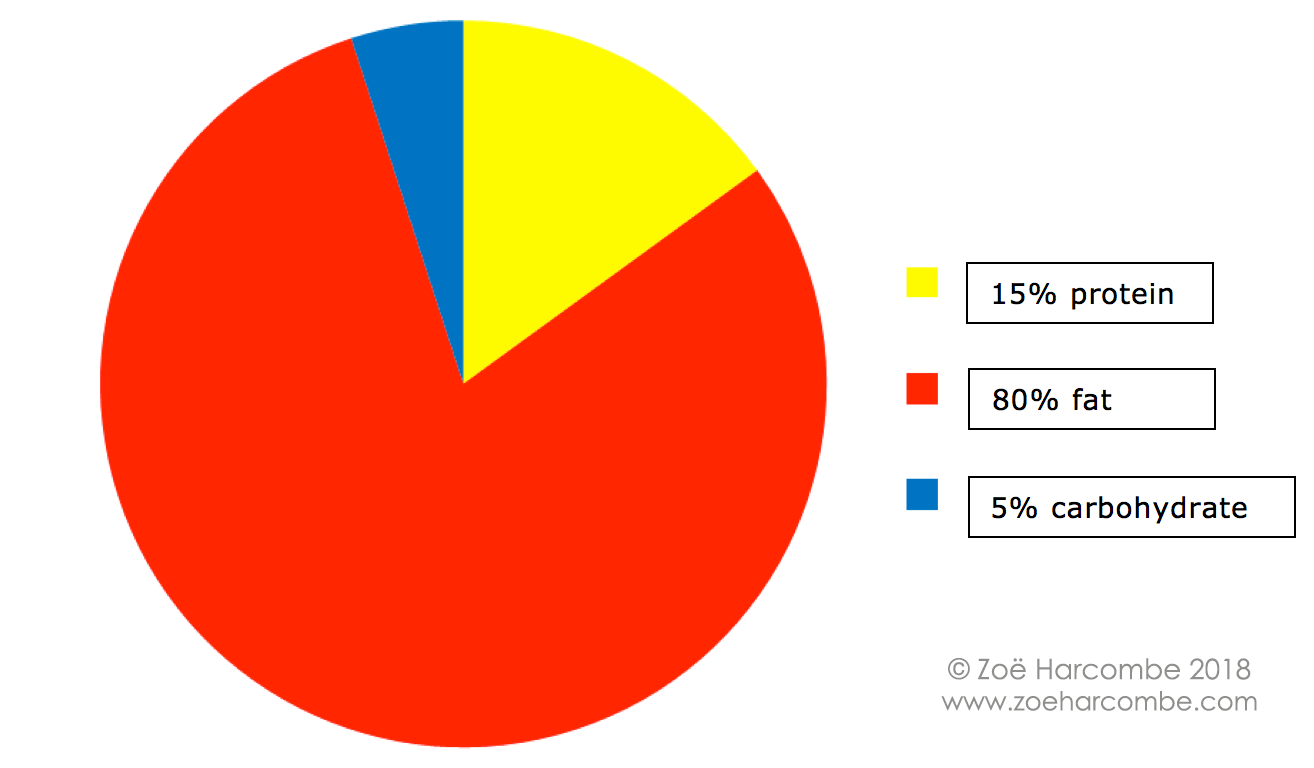
However, and this is where butter comes in, consuming a diet with the macronutrient ratios 5% carb, 15% protein and 80% fat can be quite unnatural. It involves adding dietary fat – the palatable options are usually butter and/or coconut oil and butter is generally more readily available.
A typical LCHF day

Let us assume that someone is trying to follow what I call ‘hard-core’ LCHF – macronutrient ratios of 5% carb, 15% protein and 80% fat. A person could pick any one of these and the other two macronutrients would be determined by the ratios. e.g. Most commonly LCHF people limit carbohydrates by grams. If a person sets a carbohydrate intake of 25g (grams) a day, carbohydrate has approximately 4 calories per gram, so 100 calories of carbohydrate would be consumed. If this is 5% of daily intake, then total intake is 2,000 calories. 15% of those 2,000 calories (300) would then come from protein (75g of protein at approximately 4 calories per gram) and 80% of those calories (1,600) would come from fat (178g of fat at approximately 9 calories per gram.)
The Optimal Diet, which I covered here (Ref 7), uses protein as the starting point. The ideal protein intake was calculated by the creator of The Optimal Diet, Jan Kwasniewski, on the basis of what he called “due body weight”. Due body weight, in kilograms, is estimated as a person’s height in centimeters minus 100 (± 10%). Thus, for a person 160 cm tall, a due body weight is 60 kg ± 6 kg. Kwasniewski then used the usual approximation that people need 1 gram of protein per kilogram of body weight to establish that the 160cm person needs 60 grams of protein ± 6 grams. The due body weight takes into account the protein need for where we want our weight to end up – not where it is now. (Taking height in cm and subtracting 100, by the way, is a pretty good rule of thumb for getting a weight in kg in the normal BMI range.)
The Optimal Diet used the protein intake in the following formula to establish what the intake of carbohydrate and fat should be:
1 gram of protein : 2.5-3.5 grams of fat : 0.5 grams of carbohydrate. (A fat range was given to allow for more active/slimmer people needing more energy).
A worked through example of The Optimal Diet, for a person 160cm tall, is shown below (using the lower fat range):
Example – lower fat range (2.5x)
| Breakfast |
Grams |
Cals |
Carbs (g) |
Fat (g) |
Protein (g) |
| 2 large eggs (Ref 8) |
100 |
143 |
1 |
10 |
13 |
| Bacon (Ref 9) |
50 |
209 |
1 |
20 |
6 |
| Milk, whole, 3.25% (Ref 10) |
200 |
122 |
10 |
7 |
6 |
| Lunch | |||||
| Butter, without salt (Ref 11) |
90 |
645 |
0 |
73 |
1 |
| Dinner | |||||
| Lamb (Ref 12) |
175 |
506 |
0 |
42 |
29 |
| Broccoli, raw (Ref 13) |
100 |
34 |
7 |
0 |
3 |
| Cauliflower, raw (Ref 14) |
100 |
25 |
5 |
0 |
2 |
| Beans, green raw (Ref 15) |
100 |
31 |
7 |
0 |
2 |
| TOTAL (may be rounding errors) |
1,715 |
30 |
151 |
61 |
|
| Target (lower fat range) |
1,710 |
30 |
150 |
60 |
|
| As a % (macronutrient ratios) |
7% |
79% |
14% |
The Optimal Diet formula, using the lower end of the fat range, delivers a diet made up of 7% carbohydrate, 14% protein and 79% fat, which is close enough to the 5% carbohydrate, 15% protein and 80% fat in the pie chart above. You can see from the table that very little veg is consumed, which provides the carbohydrate. Meat needs to be richer in fat than protein (fish/chicken don’t feature in ‘hard core’ LCHF). Three normal meals a day is not really possible with carbohydrate and protein restriction and butter (or another fat) needs to be consumed to get the fat intake close to 80%. (The butter would likely be added to breakfast/dinner and lunch skipped).
Butter – nutrition
I’m aware that I’m about to head into controversial territory. Butter is seen as a health food in the LCHF community and I don’t even think of it as a food. It is absolutely one of the best fats to cook with – because it is stable (I call it stable fat, not saturated fat) (Ref 16). It is definitely healthier than ‘unstable’ margarines and spreads for any purpose. But, gram for gram, in terms of nutrition, there is usually a better real food that could be consumed.
The US Department of Agriculture all foods database is my go-to reference for nutrition data. With the caveat that butter from grass fed animals would be more nutritious than the butter analysed on the USDA database, per 100g, butter is: 81g fat (51g saturated/stable fat and the rest unsaturated/unstable fat); 18g water; 0.9g protein; and 0.1g carbohydrate (Ref 17). Per 100g, butter contains 2,499 IU of vitamin A (for 717 calories); chicken liver contains 11,077 IU of vitamin A for the same weight (100g) and 116 calories. Per 100g, butter has 2.3mg of vitamin E; sunflower seeds contain 33.2mg of vitamin E for the same weight (100g) and 584 calories. Butter provides negligible amounts of calcium, phosphorus and other vital minerals.
Butter, it is argued, contains healthful short and medium chain fatty acids, and it does. But cheese – especially goats’ cheese – also contains good amounts of butyric acid, caproic acid, caprylic acid, capric acid, lauric acid etc and cheese is almost as good for the fat soluble vitamins, better for the B vitamins and far better for minerals (Ref 18). That’s gram for gram – cheese fares even better vs. butter calorie for calorie. The meat and milk from ruminants (cows, sheep, goats) also contain nutrients found in butter.
Adding butter to food
I first saw someone adding butter to their meal when I spoke at a LCHF conference in Norway in November 2014. Andy and I dined with other speakers the evening before the conference. We were in a top class fish restaurant in Oslo – enjoying local oily fish delights from herring to gravlaks – when I noticed the very slim, tall male opposite me asking the waiter for extra butter, which he proceeded to layer on top of his fish. We were with this male for much of the weekend and, at every meal, he added butter to his meat and eggs. He didn’t bother much with veg. This was our introduction to LCHF.
I then spoke at the LCHF conference in Cape Town in February 2015 and again saw some very slim people (mostly male) adding butter to meat/eggs (they chose the fattiest meats on the menu, not fish/chicken), while largely avoiding vegetables, let alone other carbs. I asked why this was being done and the answer I got was – this is how I manage my diabetes (all the people I met were type 2, but I know some type 1s do this too). The rationale for diabetes is that we know carbohydrate impacts blood glucose and insulin. We know, not least from the work of Holt (Ref 19), that protein impacts insulin. Dietary fat doesn’t impact blood glucose or insulin (Ref 20). Fat is thus the safe macronutrient for diabetics. I could see that these lean diabetics, most of them also athletes, needed to add dietary fat to their food. This was the only way for them to consume enough energy to function and to not waste away, while keeping their diabetes in remission. It was fascinating and enlightening.
However, at both conferences and a number of times since, I have observed overweight and obese people adding butter to their food. I have repeatedly advised people trying to lose weight in our on-line club not to do this. Videos like “Butter makes your pants fall off” (Ref 21) and general promotion of butter as a weight loss tool within the LCHF community seem to have made people think that the mere act of adding butter to food will make your pants fall off! However, I wonder how many people who saw the “Butter makes your pants fall off” video also saw the subsequent warnings from ‘butter man’, Bob Briggs, not to eat sticks of butter (Ref 22).
If the butter intake in the example table above were halved, the macronutrient ratios would be 9% carb/17% protein and 74% fat. The fact that the ratios have changed slightly should not be a concern – no more carbohydrate or protein has been consumed and so macronutrients that impact upon diabetes are unchanged. There’s just less eating butter ‘for the sake of it’.
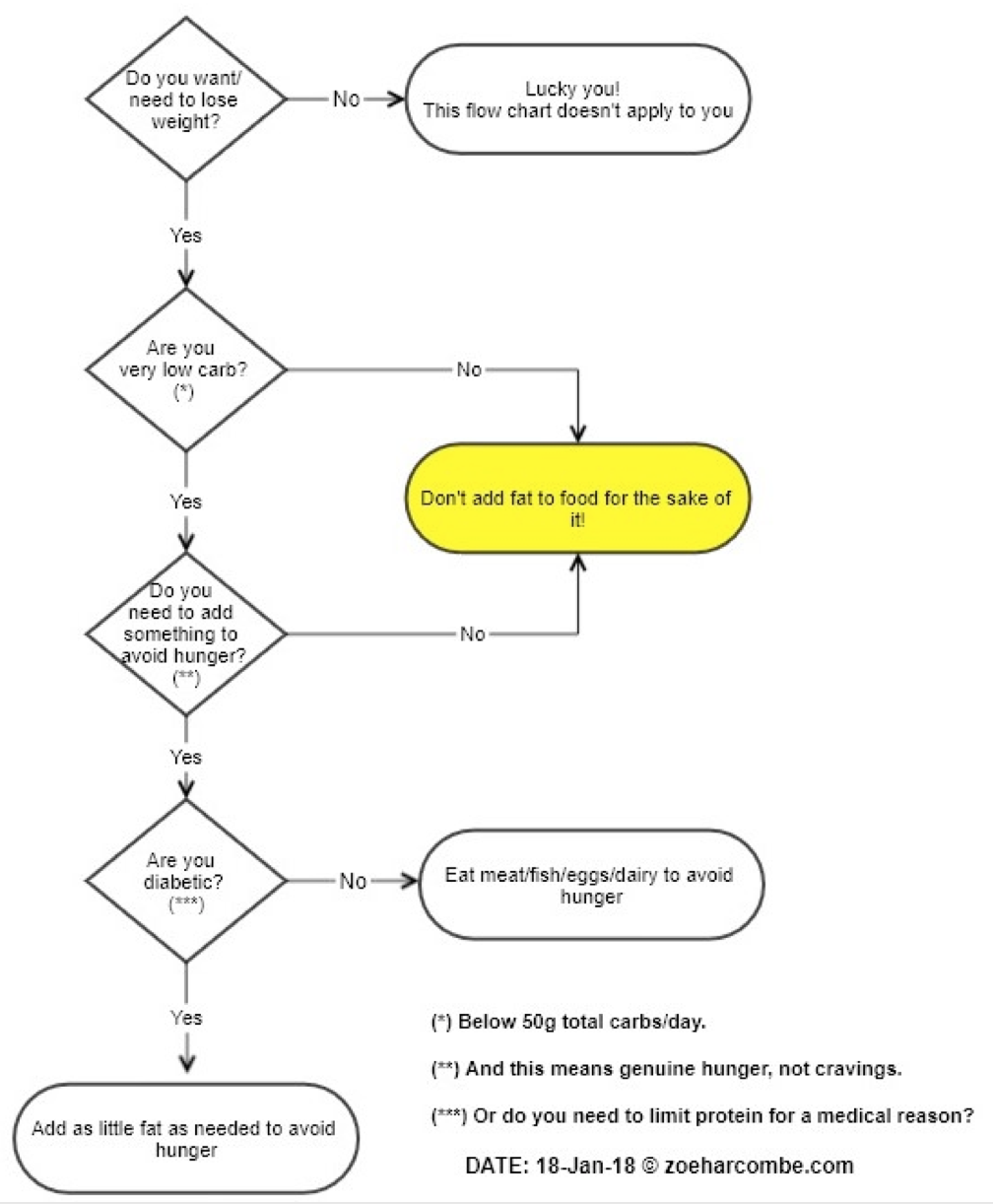
If you are like the lean diabetics I have met at conferences and you’re adding butter to very low carb, low protein, real food to maintain weight and energy, keep up the great work. However, if you want/need to lose weight, you might like to follow this flow diagram:
Will someone lose weight following The Optimal Diet to the gram (including 90g – or your own height equivalent – of butter)? The answer is probably. But I haven’t seen much awareness of The Optimal Diet formula, let alone rigid adherence to the precise macronutrient grams that it mandates. Instead, I see obese people randomly adding large chunks of butter, on top of the same meal that I’m having, ‘for the sake of it’. I’m suggesting that this is not a good idea.

References
Ref 1: Dehghan M, Mente A, Zhang X, et al. Associations of fats and carbohydrate intake with cardiovascular disease and mortality in 18 countries from five continents (PURE): a prospective cohort study. The Lancet 2017.
Ref 2: https://www.zoeharcombe.com/2017/09/the-pure-study/
Ref 3: Harcombe Z. Dietary fat guidelines have no evidence base: where next for public health nutritional advice? Br. J. Sports Med. 2016.
Ref 4: Gordon Wardlaw, Smith. A. Contemporary Nutrition. Seventh edition ed: McGraw Hill, 2009.
Ref 5: The UK report did note that 30% was likely a step too far and that 35% could be an interim goal, but 30% was the end goal.
Ref 6: Carter J.P. Eating in America; Dietary Goals for the United States; Report of the Select Committee on Nutrition and Human Needs US Senate. Cambridge, MA, USA: MIT Press 1977.
Ref 7: https://www.zoeharcombe.com/2017/04/the-optimal-diet/
Ref 8: http://nutritiondata.self.com/facts/dairy-and-egg-products/111/2
Ref 9: http://nutritiondata.self.com/facts/pork-products/2208/2
Ref 10: http://nutritiondata.self.com/facts/dairy-and-egg-products/69/2
Ref 11: http://nutritiondata.self.com/facts/dairy-and-egg-products/133/2
Ref 12: http://nutritiondata.self.com/facts/lamb-veal-and-game-products/4783/2
Ref 13: http://nutritiondata.self.com/facts/vegetables-and-vegetable-products/2356/2
Ref 14: http://nutritiondata.self.com/facts/vegetables-and-vegetable-products/2390/2
Ref 15: http://nutritiondata.self.com/facts/vegetables-and-vegetable-products/2341/2
Ref 16: https://www.zoeharcombe.com/2016/05/types-of-fat/
Ref 17: http://nutritiondata.self.com/facts/dairy-and-egg-products/133/2
Ref 18: http://nutritiondata.self.com/facts/dairy-and-egg-products/144/2
Ref 19: Holt SH, Miller JC, Petocz P. An insulin index of foods: the insulin demand generated by 1000-kJ portions of common foods. The American journal of clinical nutrition 1997.
Ref 20: Falko JM, Crockett SE, Cataland S, Mazzaferri EL. “Gastric inhibitory polypeptide (GIP) stimulated by fat ingestion in man.” J Clin Endocrinol Metab. 1975. (https://www.ncbi.nlm.nih.gov/pubmed/1159045)
Ref 21: https://www.youtube.com/watch?v=h6aMN6NLOTQ
Ref 22: http://www.buttermakesyourpantsfalloff.com/no-dont-eat-sticks-of-butter/



60g a protein a day is far too low. How can anyone find that satiating? I certainly don’t. I probably get at least double that.
As for eating a plate of butter for lunch? Ugh. I tried adding butter to food it made me very ill.
I eat low carb and the advice is always eat more fat. Starving yourself seems stupid. Doing that to hopefully trick the body into eating itself? Good luck!
And the keto dudes always advocate eating more fat. Everyone on their forums says the same thing
Hi Zoe,
My son is type 1 diabetic. I have recently reduced his carb intake to 75 g per day which is down from 300 g a day and an amount he will not fight me on for now. He is overweight, not obese though. Last week at our paediatric diabetes clinic appointment, the dietician told me that carb amount is too low. She says that 50 – 55% of carbs of caloric intake of 2000 a day is required for his healthy brain development. She said that if I continued on the low carb for him that I would see his school performance suffer and he would not develop normally. My decisions have been influenced by Richard Bernstein’s work in the field and by research that reports on the Ketogenic diet as treatment for children with epilepsy. My argument for the dietician is that if these children are lower than 20 g a day and no significant interruption to normal brain development was noted, 75 g a day should be a walk in the park for my son’s brain. Do you have any insights or research that helps to support or challenge my thinking here? I am fairly certain that adequate protein would supply my son’s brain with the glucose requirements through gluconeogenesis. Any insights you could share would be very greatly appreciated. Thanks!
Hi Jill
Oh the ignorance of dieticians!
Thank you for asking for insights and not advice because I can’t give advice. I am a huge fan of Bernstein’s work. I think you’ve reached a really sensible and pragmatic position – not going as low as Bernstein recommends, but finding a level that works for your son. Top idea in my view!
You’re right with your argument. To give you added insights, here are the notes that I made watching the brilliant Dr Eric Westman at the Cape Town conference in Feb 2015.
Eric first reminded us that “The lower limit of dietary carbohydrate compatible with life apparently is zero, provided that adequate amounts of protein and fat are consumed.” I had been familiar with that reference for some time – it’s here p275 (http://www.nap.edu/catalog/10490/dietary-reference-intakes-for-energy-carbohydrate-fiber-fat-fatty-acids-cholesterol-protein-and-amino-acids-macronutrients).
Eric then went on to say – the brain is not an obligate carb user although this is still taught. Dieticians say “because the brain uses 120g carb you must ingest 120g of carb.” Gluconeogenesis means that the body can make glucose. 80% of the central nervous system energy can be derived from ketones leaving c. 20-28g of glucose a day that is really required by the brain. He continued – endogenous glucose production occurs at a rate of approximately 2-2.5mg/kg/minute -> 2.8-3.6g/kg/day. In a 70kg man this represents 210-270g/day. There is no need to ingest glucose, but the 20-30g a day consumed by people on ketogenic diets is helpful.
As the sister of a T1D now suffering serious problems as a result of the 55% carb advice, I wish our mum had read Bernstein. She does too :-(
Best wishes – Zoe
This is extremely validating. Thank you so much, Zoe. <3
Jill
http://typeonegrit.blogspot.co.uk
would be a good resource, from what I have read
Also search on Troy Stapleton, a low carb Type 1 doctor.
“She said that if I continued on the low carb for him that I would see his school performance suffer and he would not develop normally.”
That would make him ideally qualified to become a dietician then. (Well someone had to say it)
Zoe, If I believe my relatively low carb meals (twice a day only, 7 – 9 hr eating window) is too low in fat (maybe I am still peckish), then I prefer to take a desert spoon or 2 of EVOO rather than butter.
Thanks R
BHi Robert
I personally think butter would be better than EVOO. There are benefits in the short and medium fatty acids, as mentioned in this article. EVOO has a couple of fat soluble vitamins and not much else (butter is slightly better, but not a good as cheese/meat/eggs/fish, as shared in the article). However, it’s not a big deal – if EVOO works for your health goals – keep up the good work!
Best wishes – Zoe
Ola Zoé
Parece-me que há limitação de proteinas por refeição – questão da absorção.
Sabe me dizer quais esses limites, considerando o peso da pessoa?
Hi Beto
This translates to: “Hi Zoé It seems to me that there is limitation of proteins per meal – matter of absorption. Can you tell me what those limits are, given the weight of the person?”
The answer is in the post – it’s set by the Optimal Diet formula: “The Optimal Diet, which I covered here (Ref 7), uses protein as the starting point. The ideal protein intake was calculated by the creator of The Optimal Diet, Jan Kwasniewski, on the basis of what he called “due body weight”. Due body weight, in kilograms, is estimated as a person’s height in centimeters minus 100 (± 10%). Thus, for a person 160 cm tall, a due body weight is 60 kg ± 6 kg. Kwasniewski then used the usual approximation that people need 1 gram of protein per kilogram of body weight to establish that the 160cm person needs 60 grams of protein ± 6 grams. The due body weight takes into account the protein need for where we want our weight to end up – not where it is now. (Taking height in cm and subtracting 100, by the way, is a pretty good rule of thumb for getting a weight in kg in the normal BMI range.)
The Optimal Diet used the protein intake in the following formula to establish what the intake of carbohydrate and fat should be:
1 gram of protein : 2.5-3.5 grams of fat : 0.5 grams of carbohydrate. (A fat range was given to allow for more active/slimmer people needing more energy).”
I hope that translates back OK!
Try: “A Dieta Ótima, que abordei aqui (Ref 7), usa a proteína como ponto de partida. A ingestão ideal de proteínas foi calculada pelo criador de The Optimal Diet, Jan Kwasniewski, com base no que chamou de “devido peso corporal”. O peso corporal devido, em quilogramas, é estimado como altura da pessoa em centímetros menos 100 (± 10%). Assim, para uma pessoa de 160 cm de altura, um peso corporal devedor é de 60 kg ± 6 kg. Kwasniewski usou a aproximação usual de que as pessoas precisam de 1 grama de proteína por quilograma de peso corporal para estabelecer que a pessoa de 160 cm precisa de 60 gramas de proteína ± 6 gramas. O peso corporal devido leva em conta a necessidade de proteínas para onde queremos que nosso peso acabe – não onde está agora. (Tomando altura em cm e subtraindo 100, a propósito, é uma boa regra geral para obter peso em kg no intervalo normal de IMC).
A Dieta Ótima usou a ingestão de proteína na seguinte fórmula para estabelecer o que a ingestão de carboidratos e gorduras deve ser:
1 grama de proteína: 2,5-3,5 gramas de gordura: 0,5 gramas de carboidrato. (Uma gama de gordura foi dada para permitir pessoas mais ativas / mais finas que precisam de mais energia).”
Best wishes – Zoe
I suspect that macronutrient research will start making more sense when the macro-catagory ‘protein” is ditched and 2 important distinctions made:
1) between crude protein and amino acids
2) bio-available protein
For example 100 g of animal protein is usually 90+% grams of protein in the blood. 100 g of lentil protein will be 50 to 60 grams of protein. Comparing animal protein to plant protein is comparing apples to oranges.
Zoe, great article. I struggle with good quality protein on a vegetarian diet–there is cheese and eggs. Barely tolerate the latter. I am not diabetic and am LCHF (would gladly go keto but options are few). Heard that podcast on 2 keto dudes truly inspiring–new in this game–used to be a nutritionist but gave it up to become a family physician–battling with the establishment in Oz. Rod Taylor a great inspiration too.
Hi Ira
Many thanks for your comment. I was a veggie for 20 years – had at least 2 avoidable operations during that time. Should have seen the light sooner, but at least my price was not as high as others (e.g. Lierre Keith). I still truly understand the veggie pull – you’re right to recognise the nutritional side as a challenge. Prof Noakes knows a vegan LCHF! Apparently he lives on coconut oil and supplements :-)
Good luck with your battles
Best wishes – Zoe
Hello Zoé,
I think it makes a lot of sense estimating minimum protein requirements by using height, as height is a constant. There’s a lot of conflict and confusion caused by estimating protein needs based gm per kg current weight, lean weight and ideal body weight. Height is so much simpler.
I suspect the height/protein formula would be more universal if it had a range that allowed for more protein for males and those seeking muscle gain, weight loss or athletic performance improvement. (pregnant?)
For weight loss, is there a case for having more generous upper protein limit, due to the satiating effect of protein? This may be more helpful (getting that lunchtime serve in your table) than any damage from a small insulin spike from that protein dose.
Also, I’d like to read more on the insulin response to protein (rich foods). Is there any variance with different protein sources (beef, chicken, fish, whey etc… ) or indeed between different people?
PS I too have witnessed overweight LCHF proponents adding much butter to meals and coffees. Well intended but mislead. Calories still count.
Hi Jamie
Many thanks for all these contributions. We’ve been having some Twitter debates today on Ted Naiman’s view of protein and Dr Ron Rosedale and Dr Michael Eades have v different view on protein. One argument is that it is aging; another that it maintains the body and helps to avoid the common loss of muscle with aging. I’ll bow to experts who have looked at protein and telomeres more than I have.
Protein not only has satiety for weight loss, but it is the best example of the second law of thermodynamics. More energy is lost converting protein to energy than for fat or carbs. It as a thermic advantage, therefore. One that I suspect body builders have observed, if not learned about.
This is the best paper for insulin response to different foods (not between different people) http://ajcn.nutrition.org/content/66/5/1264.abstract
Best wishes – Zoe
I agree with your analysis of the nutrients/calories in butter. But I eat a lot of butter in order to control my protein while eating to satiety. I’ve been off sugar-grains-lentils since 2011 so I’m not a newbie. For some time I ate 90% fat/oil and found myself eating 45 g of protein/day and pretty skinny at 68 kg. That was a fun experiment. I decided to try to eat more protein so reduced fat to 85%. I was able to eat more protein, 60-70 g. (178 cm tall, 69 years old) Then I dialed fat back further to 75% and find myself eating around 90 g of protein. As fat goes down and protein up, weight goes up. If I maintain 75% for another month, I’ll probably hit 75 kg. I cook with straight up animal fat like suet/lard along with meat but it still takes added oil to hit 75% fat. Eggs are 65% fat. Just enough butter to cook them might make that 70%. If I ate to satiety at 70% fat, my protein consumption would probably cross 100 g. That seems excessive for my height/weight. I walk 7 km every day, no other exercise. So how am I to trade in butter for more nutrients without going over the top in protein?
Hi Tim
Stick with butter! You bow out at the first question in the flow chart “Do you want/need to lose weight?” No = lucky you!
Best wishes – Zoe
Is this argument back-to-front? I don’t calculate everything, I make a meal and eat it. I am trying to be very low carb. So if I add butter to a breakfast for instance, I am trying to get a balance – eating less of something else by adding butter to bulk it out. So long as I gradually lose weight and my blood glucose stays in control I think I am close enough to the mark.
Hi Aidan
If you’re continuing to lose weight, keep up the good work. You could eat something more nutritious than butter, however. If you’re diabetic, and so need to watch protein, fair enough, but if not – is butter the most satiating and nutritious choice?
Best wishes – Zoe
When I examine various guidelines for what we should be consuming, I often think “they are not talking about me”!
I’m ApoE-3/4. I believe ketosis is a good food-style for neurological mitochondrial health.
I’m age-70, after many years of sarcopenia. I think I need more than average protein (plus exercise).
I’m BMI-19, thin outside & inside. Good A1C, low TG/HDL ratio, and probably very low IR.
I don’t count calories or measure macros. What’s the point if I don’t know what they should be for ME?
I believe my best policy is to measures RESULTS, not INPUTS. Am I in ketosis? Are my A1C and TG/HDL (etc) numbers good? Is my BMI stable? Do I enjoy my food and feel satiated and never suffer “hanger”? (I like cooking with plenty of butter, etc. But I don’t add EXTRA butter).
People differ massively. I think I’m an outlier, and I need my own guidelines. I’m not the only one.
4/4 here. Meaningful info about apoe genotype is sparse indeed on the ground. I wish I understood more!
Hello Zoé
An interesting blog. Older people I am told are quite often protein déficient in their diets, which has á side effect of muscle loss. Looking at my protein intake, I found I was nowhere near the 1 gm per kilo of body weights , so I havé started taking á protein supplement in the form of whey. A good idea?
Hi Chris
I would be really surprised if anyone eating real food is deficient in protein. As an example, for my 50kg, I need 50g protein a day and I would get that in a reasonable size tuna steak. That’s aside from the fact that I would get protein in every single other thing that I eat from lettuce to berries to yoghurt to stir fry veg to meat/eggs etc.
Try inputting a typical day one of these diet analysers and see where you end up. There are some nasty ingredients in these protein shakes – a glass of milk would be so much better!
Best wishes – Zoe
Hi Zoe – interesting that you found LCHF the same year that I did, because your writing and information has been a true light to me along my own LCHF way these past 4-5 years. I (and my husband) respect your work so much I became a subscriber, and definitely feel the subscription is worth every penny. You’ve given us so much good information, and continue to do so, that this comment about seniors and protein gives me a chance to perhaps share some information with you.
My experience with the seniors in my own life is that they probably think they are eating real food, but what they eat ends up looking protein deficient to me. They eat out a lot, and restaurants are quick to fill patrons up with cheap commodity carbohydrates: bread, potatoes, pasta. I personally don’t consider white bread a real food, but many people must, because they’re eating tons of sandwiches with it. And, there’s very little protein in a McDonald’s lunch, for example. You and I may not eat that way, but many many people do. And when we dismiss comments about adequacy of protein, this gives other people permission to do so also.
Some sobering information about protein adequacy, at least in the US, and keep in mind that these are based only on the USDA’s bare minimum protein recommendations, which are 56 g/day for men, and 46g/day for women – well below the 60-70 g/day numbers discussed in comments above:
Most WOMEN, not just seniors but women generally over the age of 8 do not meet this minimum of 46 g/day, according to NHANES data. As you know that’s the threshold for avoiding malnutrition and I have to wonder if osteoporosis and osteopoenia could be related to this deficiency. I also wonder how much this contributes to sarcopenia and falls, and injuries from falls – and then poor healing afterwards, since the body needs more protein when it’s healing. If the USDA were to implement the height-based suggestion, and the average woman is 5’4″ if memory serves, or 162 cm, and a recommended intake of 62 g of protein, how big would the percentage deficent be then? Just larger, or MUCH larger?
About 50% of males look to be hitting this (ultra-low, IMHO) number, and another 20-25% are just “meeting” the recommendation. 50% not hitting it is warning enough. But, and, if the recommendation is low to begin with, then that intake that they are calling barely adequate is low also. The average man in the US is 5’10”, I believe, which is 178 cm, so your suggested calculation – which I like for its simplicity – is 78 g protein. The majority of senior men are getting just 56 g/day, or below. That’s definitely deficient.
The NHANES data I cite come from here:
https://health.gov/dietaryguidelines/2015-scientific-report/06-chapter-1/d1-11.asp#figure-d1-20
Thank you again for all your wonderful, tireless work, and I hope I may contribute something to it through this post or at least through my subscription. Please keep cracking on, the world needs you!
Hi Wendy
Thank you so very much for your kind words and support for my work. I couldn’t do what I do without people like you – I’d be back being an HR Director!
Thanks so much for the data too – I’ll take a look at that. It should be difficult to be deficient in protein (unless vegan/veggie) but, as you say, unless you eat real food, it’s entirely possible!
Best wishes – Zoe