
How statin drugs really lower cholesterol & kill you one cell at a time
Introduction
(Jump to the Executive Summary at the end if you don’t want the full monty).
This is a review of a book written by James & Hannah Yoseph entitled How statin drugs really lower cholesterol: and kill you one cell at a time (and many thanks to Eric who posted a comment to say that there is a ‘made easier’ version of this here.)
I won’t reiterate the importance of cholesterol – you can read this on this post. Suffice to say your body makes cholesterol because it is so utterly vital, the body cannot leave it to chance that you would consume it. You would die instantly without cholesterol – it is a fundamental part of every cell in your body.
This book should be read by every person BEFORE they either prescribe or take statins. I would be interested to know if any person could prescribe or take statins AFTER reading it…
There is an interview with the Yosephs here.
The three key contributions of the Yoseph book
There are three key contributions of this book:
1) The explanation of precisely how statins work in the human body (and in animals where they have been used for drug testing).
2) The documentation of medical journal articles proving that the precise mechanism as to how statins work has been known by their proponents throughout.
3) The detailing of the conflict of interest endemic in the pharmaceutical industry and approval processes, which have monumentally failed the human race. The book takes one drug company, Merck, and the American Food & Drug Administration (FDA) and a number of other related bodies (e.g. the National Cholesterol Education Programme NCEP) and a handful of individuals and traces in incredible detail the role that each played in this scandal. And it is a scandal.
Let us look at the three main findings that the Yosephs have given us:
1) How statin drugs really lower cholesterol
Every cell needs sustenance. The cell says “I’m hungry” and makes a protein called “reductase.” Reductase activates something called the mevalonate pathway. Mevalonate is cell food just as glucose is brain food. Mevalonate is utterly vital for the life of every cell in the human body.
The Yoseph’s put it this way: “Mevalonate is the essence of cell renewal. In all cells, mevalonate travels down the mevalonate pathway to make cholesterol and isoprenoids (five-carbon molecules). Both stimulate the cell to grow, replicate its DNA and divide into two cells. This is the ‘cell cycle’. This is life.”
Cell renewal is continuous throughout the body – cells lining the gut are turned over every 10 hours to 5 days; skin cells are recycled every two weeks; liver cells are replaced every 300-500 days and bone cells last a decade.
Without the cholesterol and isoprenoids made by the mevalonate pathway, none of this cell rejuvenation happens. Isoprenoids make our cells replicate and renew. Without mevalonate and without isoprenoids, cells age and die. They cannot be replaced.
CoQ10 is an isoprenoid. CoQ10 is vital for cell energy. Heme-A is an isoprenoid. Heme-A is vital for cell energy and drug metabolism. Isopentenyl adenine is an isoprenoid. Don’t worry about the names in all of this – just remember that Isopentenyl adenine is vital for DNA replication. DNA is the blueprint of every cell. Before a cell divides, it replicates its DNA and the new cell can be formed from the same blueprint. There are other vital isoprenoids – all are stopped from functioning by the disruption of the mevalonate pathway.
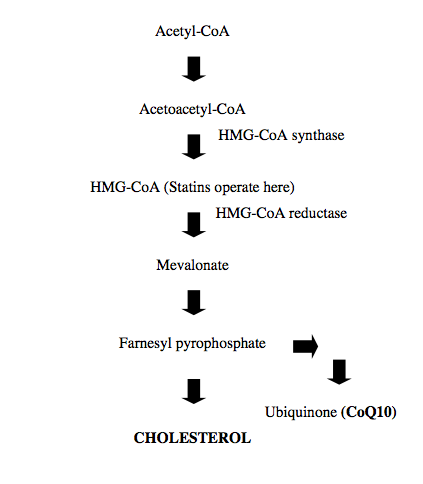
In the simplified flow chart above, showing the cholesterol production pathway in the body, we can see why statins are called HMG-CoA Reductase inhibitors – this is the part of the pathway that they disrupt. Statins disable reductase. Without reductase, the mevalonate pathway cannot function properly. Without the mevalonate pathway, cells cannot rejuvenate properly. It follows that the life of every cell in the human body is catastrophically impaired by statins.
How long does it take cells to be affected? That depends on the life cycle of the cell – 300-500 days for liver cells and up to 5 days for the cells lining the gut.
In chapter four of the Yoseph’s book there is one of the most incredible explanations about what statins actually do, which I have not seen elsewhere. The Yosephs describe the fact that statins are not just HMG-CoA reductase inhibitors, they are also reductase stimulators…
Life preserving responses are hard wired at the cell level – our body will do whatever it takes to keep us alive; every cell will do its bit to keep us alive. Because reductase is the ‘food’ for cell reproduction, taking something that impairs this process (statins) triggers the body to try to overcome the damage that is being done. Reductase production increases to try to reopen the mevalonate pathway. It’s a terrific attempt by the body to fight back. However, the Yosephs sadly note: “So far, they have not figured out how to save statin-fed dying cells except by adding back mevalonate.”
The book describes that there are two ways in which every cell of the body can get the cholesterol it so vitally needs: 1) it can make cholesterol and 2) it can take cholesterol from the blood stream.
When someone takes statins, the cells are impaired from making cholesterol so they try to take the cholesterol from the blood stream. The LDL receptors on each cell go into overdrive and try to ‘receive’ more LDL from the blood stream to compensate for the fact that the cell can’t currently make as much itself. This lowers the cholesterol in the blood stream. (Please remember that LDL stands for Low Density Lipoprotein – it is not cholesterol, let alone bad cholesterol. Similarly HDL stands for High Density Lipoprotein – it is not cholesterol, let alone good cholesterol).
That’s how statins lower cholesterol and that’s how statins kill us one cell at a time.
Familial Hypercholesterolemia (FH)
It is time to mention Familial Hypercholesterolemia (FH) here. FH is a genetic condition caused by a gene defect on chromosome 19. The defect makes the body unable to remove LDL from the bloodstream, resulting in consistently high levels of LDL. Bearing in mind that FH is rare to start with – one in 500 people – in some cases of FH the LDL receptors work to an extent (just not very well); in other cases the LDL receptors work barely at all.
My logical consideration of FH suggests to me that the problem is that the LDL receptors don’t work properly and therefore the LDL (lipoproteins) cannot get into the body’s cells in the way that they are supposed to. This means that cells don’t get the vital LDL, carrying the vital protein, lipids and cholesterol needed for the cell’s health. LDL in the blood stream is high because the LDL has stayed in the bloodstream and has not been able to get into the cells – where it is supposed to go. Hence high LDL blood levels are the sign that someone has FH. The high LDL levels are, however, a symptom and not a cause or a problem per se. The problem is that the health of every cell is compromised by LDL not getting to the cell. This includes heart, brain and muscle cells – all cells. An FH sufferer can therefore have heart problems – because of too little LDL reaching the heart cells – not because of too much LDL! How differently things can be seen when one is not blinded by thinking that cholesterol or lipoproteins are bad.
This also explains why high HDL would be seen as good. HDL is the lipoprotein that carries used lipids and cholesterol back to the liver for recycling. If the LDL were not able to get to the cells to do its job then there is little for HDL to carry back to recycle. Hence HDL would be low and this would be seen as bad with impaired understanding as to why.
Ironically, the most serious form of Familial Hypercholesterolemia would receive no benefit from statins anyway. As the extreme form of FH is characterised by LDL receptors working barely at all, even the body going into crisis mode, and trying to take LDL from the blood stream with increased LDL receptor activity, will not work if the LDL receptors are not working well enough in the first place. Hence the LDL will stay in the blood stream with an extreme sufferer of FH and yet the statin has reduced what little chance the FH sufferer’s body had of making cholesterol within the cell. The FH sufferer should ideally be given medication (if anything existed) to stimulate cholesterol production within the cell, so that the cell would at least get the vital cholesterol it needs, even when it couldn’t get it from the blood stream.
2) What was known by whom and when as statins were pushed through to approval?
We need to introduce some key players here:
– Brown & Goldstein were awarded a Nobel Prize for their work with lipoproteins. We will see what they knew along the way and their involvement with statin approval.
– Akira Endo was a Japanese biochemist who graduated from Tohoku University in 1957 and joined Sankyo Pharmaceuticals in Tokyo. Endo is the guy who discovered the poison that statins are made of. In 1971 he began his search for a fungal mycotoxin that would lower cholesterol. (Definition: “Mycotoxins are secondary metabolites produced by microfungi that are capable of causing disease and death in humans and other animals”). (A metabolite is a small molecule produced during metabolism.)
In 1976 Endo managed to extract something called citrinin, a disease-causing mycotoxin from Penicillium Citrinum. He discovered that citrinin lowered blood cholesterol and published a report on this. In the same year he abandoned his work with citrinin because it was too toxic. He extracted another mycotoxin from Penicillium Citrinum called “ML-236B”, which was less toxic but still lowered cholesterol. ML-236B became Endo’s first experimental statin. (There’s a great story in the book about how Sankyo, with Japanese cultural traits of trust and honour, approached the American drug company Merck to develop the statin together. Merck shafted Sankyo and Endo was wrongly seen as the betrayer and was ostracised by Sankyo). Endo was then ‘out on his own’ and he approached Brown & Goldstein, seeing the work that they were doing with lipoproteins, and this is how these guys got together.
(Also – if you are thinking that Penicillium Citrinum sounds like an antibiotic, you’d be right. The book states “Statins – secondary fungal metabolites – are anti-life or anti-bios. Statins are antibiotics. Because antibiotics are anti-bios and kill ‘good’ vitamin-producing bacteria in the gut, most are prescribed for as short a term as possible. Statins, on the other hand, are often prescribed for life. Most antibiotics also have specific action on specific microbes. Not so with statins. Statins indiscriminately kill any cell including human cells.” (Their emphasis). This could explain the warnings about gut health on statin patient leaflets.)
In 1953 Watson and Crick discovered the structure of DNA. In 1979 Marvin Siperstein discovered that DNA replication (cell rejuvenation) required isoprenoids from mevalonate (specifically the isoprenoid called isopentenyl adenine). (p10 in the book) (I won’t dwell on Marvin Siperstein, but he’s one of the good guys in the Yoseph book – writing his important discoveries and highlighting serious issues in medical journals. These articles were sadly ignored.)
In 1976, Beecham Labs in the UK (what became SmtihKline Beecham and then Glaxo SmithKline) had discovered a statin named “compactin”. Sankyo Pharmaceuticals had discovered the same compound in parallel in Japan. They called it Mevastatin. “Stat” in statin means to stop and mevastatin means “to stop mevalonate”. So they knew exactly what they were stopping when they named this drug. Within an hour of adding compactin to cholesterol-rich cells, the cell reproduction cycle was completely stopped. Within minutes of adding back a small amount of mevalonate, DNA replication and cell cycles were completely restored.
This bit is key – because the cells were given ample cholesterol before the experiment (they were “cholesterol-rich cells”), it was clear that the problem was not cholesterol deprivation but isopentenyl adenine deprivation (that isoprenoid that enables DNA replication). The absence of this isoprenoid prevented DNA replication and the entire cell cycle.
As the Yosephs state “Cells are poisoned by statins because statins block the making of isoprenoids from mevalonate. If cells cannot replicate, they inevitably die.”
In 1977 (p37 of the Yoseph book), Endo, Brown and Goldstein published a paper documenting that statins caused an increase in reductase. It was therefore known back this far that statins should not necessarily be called reductase inhibitors, but reductase stimulators. They didn’t detect the increase in LDL receptor activity at this time.
In 1978 Merck developed their own statin.
In 1979 Endo patented another statin and sold it to Sankyo to try to restore his honour.
On p143 of the book, The Yosephs present an image of a paper written by Brown and Goldstein in The Journal of Biological Chemistry (1979). This incredible quotation from their paper is extracted: “Mevalonate, the product of HMG-CoA reductase, also supported growth, confirming that compactin was exerting its killing effect by a specific inhibition of HMG-CoA reductase.” So Brown and Goldstein admitted that the first statin, compactin, had a killing effect and this was a result of inhibiting reductase. They went on to develop further statins, which also inhibited reductase and also had a killing effect.
In 1980, Brown and Goldstein wrote the following in The Journal of Lipid Research (we’ll see who’s behind this journal shortly): “When the regulator of reductase is identified, it may be possible to administer this compound to animals and perhaps to patients, preventing the compensatory rise in reductase…” Hence Brown and Goldstein knew by 1980 that statins both inhibited and stimulated reductase. They also knew that the “compensatory rise in reductase” was something to be prevented.
In 1980, Brown and Goldstein co-authored a paper in The Journal of Biological Chemistry stating: “CoA reductase is inhibited by compactin, mevalonate formation is blocked and cultured cells die.” (p14)
In 1980, Brown and Goldstein co-authored a paper in The Journal of Lipid Research stating: “Incubation of cultured cells with compactin blocks mevalonate production and converts the cells into mevalonate auxotrophs.” (p172) An auxotroph is something that has lost the ability to synthesise certain substances needed for its growth and metabolism.
In 1980, Endo co-authored a paper in The Journal of Biological Chemistry entitled “Isolation and characterisation of cells resistant to ML236B (compactin) with increased levels of HMG-CoA reductase”. The extract (p146 of the Yoseph book) states: “…cholesterol alone is ineffective in preventing cell death…Addition of other mevalonate-derived metabolites to the culture medium along with cholesterol including ubiquinone [That’s CoQ10 remember], dolichol and isopentanyl adenine [that’s the isoprenoid vital for DNA replication] did not prevent the toxic effect of ML236B.” i.e. nothing we could add back to the cell, to compensate for the damage we had done, could prevent the toxic effect.
Also in 1980, Sankyo cancelled clinical trials of their statin on humans after half their laboratory dogs died of cancer. Merck called Sankyo to try to learn from this and Sankyo told them to sod off – quite right! Merck stopped statin development (sadly, only temporarily).
In 1982 Brown and Goldstein wrote in The Proceedings of the National Academy of Sciences: “If reducatase cannot increase sufficiently to overcome the inhibition by compactin, the cells die.” (p144)
Incredibly, given all of this going on, in 1982 Merck was allowed to give Lovastatin to humans in the first human trial. At this time:
– It was known that statins were toxins.
– It was known that statins blocked the mevalonate pathway.
– It was known that blocking the mevalonate pathway caused cell death.
– It was known that nothing could be added back to the body (not cholesterol, not isoprenoids, nothing) to prevent cell death and the toxic effect of statins.
– It was known that statins not only inhibited reductase, but they stimulated it too. It was known that inhibition of reductase “had a killing effect”. The consequences of stimulating reductase were not precisely known, but caused enough concern for the 1980 Brown and Goldstein article in The Journal of Lipid Research to discuss what might be administered to “prevent(ing) the compensatory rise in reductase…”
In 1984 lovastatin was approved by the FDA in record time.
In 1985 Brown and Goldstein were awarded the Nobel Prize!
3) The conflicts of interest:
We need to introduce some more players at this stage:
Daniel Steinberg
Daniel Steinberg is the overall ringmaster. If you do an internet search you will find remarkably little about him personally and this seems to be deliberate. The Yosephs should be commended for what they have managed to piece together about this orchestrator. (You will find his “Cholesterol Wars”, where he writes that “after much controversy, cholesterol and lipoproteins were implicated, indicted and ultimately found guilty.”)
Steinberg was the founder and first editor in chief of The Journal of Lipid Research (a vehicle for Endo, Brown and Goldstein and lipid theory supporters to use).
Steinberg was Chairman of the Council on Arteriosclerosis of the American Heart Association and used his position to recommend treating high cholesterol as early as 1969. (Introducing the theory that this life vital substance, made by the body, should be treated rather than revered).
Steinberg was co-chair of the Lipid Research Clinics Coronary Primary Prevention Trial (LRC-CPPT). This trial was led by the National Institutes of Health (NIH), costing the taxpayer $150 million over 13 years. In January 1984 the results were published and claimed that the long sought evidence was now available – absolute differentials were less than 2% in different groups observed.
Steinberg was Merck’s scientific advisor when lovastatin was approved in record time in 1984.
Steinberg was the first speaker at the FDA advisory committee meeting on statins, held at the NIH, in February 1987.
In 2006, writing in his own Journal of Lipid Research, Steinberg reported that “the Goldstein/Brown laboratory showed that this huge over production of reductase, representing an attempt by the cell to overcome statin inhibition, is accompanied by a huge buildup of endoplasmic reticulum, the organelle [place] in which the reductase resides. As a result the cells look “abnormal” but of course they are not cancer cells.” Steinberg admits that the cell tries to overcome what the statin is doing, he uses the unscientific word “huge” twice – neither time in his favour – and he is apparently able to single-handedly declare that abnormal cells are “of course not cancer cells”.
The same article “The discovery of statins and the end of the controversy” (how arrogant is that?!) declared: “…there was no hard evidence that compactin would be toxic in humans, only rumors about toxicity in dogs…” Rumors? Merck contacted Sankyo to understand why half their dogs had developed cancer.
Steinberg chaired the NIH consensus panel, which in December 1984 declared that LDL cholesterol was the cause of Coronary Vascular Disease (CVD) and recommended that a National Cholesterol Education Programme (NCEP) be adopted. Since this time the NCEP has set continually lower cholesterol targets. Their recommended age for statin use is now nine!
The members of the NCEP
The 2004 NCEP financial disclosure report reveals that all members of the 2004 guideline participants had received payments and/or grant funds from the following organisations:
Dr Scott Grundy: Abbott, Astra Zeneca, Bayer, Bristol-Myers Squibb, Glaxo SmithKline, Kos, Merck, Pfizer, Sankyo.
Dr Bairey: Astra Zeneca, Bayer, Bristol-Myers Squibb, Kos, Merck, Novartis, Pfizer, Procter & Gamble, Wyeth.
Dr Brewer: Astra Zeneca, Esperion, Fournier, Lipid Sciences, Merck, Novartis, Pfizer, Sankyo, Tularik.
Dr Clark: Abbot, Astra Zeneca, Bristol-Myers Squibb, Merck, Pfizer.
Dr Hunninghake: Astra Zeneca, Bristol-Myers Squibb, Kos, Merck, Novartis, Pfizer.
Dr Pasternak: Astra Zeneca, BMS-Sanofi, Pfizer, Johnson & Johnson, Kos, Merck, Novartis, Takeda.
Dr Smith: Merck.
Dr Stone: Abbot, Astra Zeneca, Bristol-Myers Squibb, Kos, Merck, Novartis, Pfizer, Reliant, Sankyo.
The members of the 1987 FDA Panel
On February 19th 1987 the FDA held an advisory committee meeting to review the NIH clinical guidelines for altering cholesterol with Merck’s new statin, lovastatin. The NIH hosted the event. This would be like the NHS hosting the approval meeting for a drug in the UK; implicit support. Incredibly a Merck consultant, Fred Singer, was in the Chair.
Steinberg and the Nobel prize winners Brown and Goldstein were present in support of Merck. The FDA advisory committee comprised 4 FDA employees, 8 FDA advisors (2 were Merck consultants) and 11 Merck speakers and guests. That put the vote 13-10 in Merck’s favour from the outset.
The Yoseph book fully documents the actual comments made in the meeting and by whom – the record was sequestered through a Freedom of Information request. A Merck toxicologist (MacDonald) admitted that rabbits on lovastatin died rapidly. He attributed this to “elevated blood levels” and got away with no one asking him elevated blood levels of what? MacDonald glossed over the fact that statins failed to lower cholesterol in rats, mice and hamsters. This was because rodents are able to reopen the mevalonate pathway – this is why they live. The rabbits couldn’t do this. This is why they died. Dogs were somewhere in between. MacDonald had to admit to liver cell damage in dogs but, again, got away with “We clearly do not understand the mechanism”. It was denied that cataracts had been observed in rats (a few cases in dogs were skimmed over).
A pharmaceutical consultant called Dr Richard Cenedella said: “I have consulted for many drug companies over the years. All of the hyper-lipidemic drugs induce cataracts in mice; it’s an early observation that holds up.” Cenedella wrote to the Journal of the American Medical Association in 1987 “…to caution against the possible complication of cataract development that might result from long-term use of this agent” [statins]
Jonathan Tobert was Merck’s Clinical Director for all trials. In March 1988 he stated that to date there had been no cataracts seen in humans taking lovastatin. The year before he co-authored a paper documenting an increase in lens opacities (i.e. cataracts) in 101 lovastatin consumers. The Yosephs pull no punches in the book. This is just one of a catalogue of examples where they are able to prove contradictory statements made by Tobert. On p121 they say “You can tell when Tobert is lying. He is either writing or his lips are moving.” And I thought I was bold!
Interestingly cataracts are back in the news as I publish this, but I have not seen any reduction in statin prescription or usage since the headlines that emanated from this JAMA research.
In April 2009 an extraordinary letter was written to President Obama by FDA scientists to say that “The FDA is fundamentally broken” and detailing examples of suppression of truth, distortion and the “FDA failing to fulfil its mission.” Nothing has happened as a result of this letter.
Conclusion
The remarkable Yoseph book has brought us the most precise understanding of how statins lower cholesterol. It has shown that the dangers were known all along – by those pushing through the launch and approval of statins. It has shown how a few key players – Steinberg, Endo, Brown and Goldstein could work with Merck and how Merck and other drug companies could infiltrate the FDA, influence the NIH and even see the establishment of a National Cholesterol Education Programme comprised of drug company funded representatives.
The scandal has been brilliant, meticulously planned and success guaranteed. Billions and billions of dollars have been generated from first demonising cholesterol and secondly discovering a poison (Definition: “Mycotoxins are secondary metabolites produced by microfungi that are capable of causing disease and death in humans and other animals”) that could stop the body making cholesterol. Or, as we now know more accurately – a poison that could drive cells to remove cholesterol from the blood stream, as those cells fight to avoid death.
The mevalonate pathway should never be blocked in a living creature. A rat may get away with it, a human won’t. If only humans died as quickly as rabbits, maybe statins would have never have been approved. The fact that they are killing us one cell at a time, but just more slowly, is little consolation.
The Executive Summary:
Cholesterol is utterly life vital. We die instantly without it. We need it for every single cell of the body, the muscles, the brain, hormones, bile production, fat digestion, reproduction – it simply cannot be emphasised enough how vital cholesterol is.
It is so vital that the body makes it – the body cannot afford to leave it to chance that we would need to get cholesterol from our diet. This makes cholesterol even more vital to the body than essential fats and protein – as we need to eat these.
Statins stop the body from making the cholesterol that it was designed to make (not entirely, or they would have an immediate 100% death rate).
Statins block something called “the mevalonate pathway”. This is catastrophic. Blocking the mevalonate pathway means that cells cannot replicate or repair themselves properly. Blocking the mevalonate pathway means that every cell in the body dies. The only thing that varies is how long each cell takes to die – some take more time than others.
Nothing can compensate for blocking the mevalonate pathway. Nothing except adding mevalonate back in to the body and we don’t do this. (We don’t even know if we can do this in humans. We shouldn’t block this pathway in the first place.) Adding cholesterol makes no difference, adding CoQ10 makes no difference. Blocking the mevalonate pathway is so flipping serious that anyone who does it should be shot. (I really think using the ‘F’ word here is quite appropriate).
The body tries to respond to the crisis that it detects. As cells realise that their ability to make cholesterol has been impaired, they try to take the cholesterol they need from the blood stream. This lowers blood cholesterol levels and ignorant doctors are happy. They know not what they have done.
There is a second way in which the body tries to save itself – it tries to increase the production of reductase, hoping that this may unblock the mevalonate pathway. It can’t. Hence reductase is both stimulated and inhibited at the same time. Who knows how the body responds to this mechanism being totally confused.
LDL receptor activity and reductase activity increase in parallel. The LDL receptors (the ‘doors’ on each cell responsible for letting LDL in to the cell, with the cholesterol and other good stuff that it is carrying) work harder to try to get LDL from the blood stream into the cells. The reductase production increases to try to reboot the mevalonate pathway, so that cells can make cholesterol as they are designed to do.
The inventors of statins knew what statins were really doing throughout the development of this drug (mevastatin literally means to stop mevalonate – they knew exactly what mevastatin would do). They knew that statins blocked the mevalonate pathway. They knew that this caused cell death. They knew that nothing could compensate for this other than putting the vital mevalonate back. They knew that CoQ10 was affected and this was serious. They patented adding CoQ10 to their statins but then never bothered to add it.
Statins were only originally intended for the 1 in 500 people with Familial Hypercholesterolemia. This would not have enabled drug companies to reach the profit potential of their dreams. Hence cholesterol has been demonised and targets have continually been reset by conflicted bodies so that the norm is no longer the norm and everyone can be told that they need statins.
Ironically, the most serious form of Familial Hypercholesterolemia would receive no benefit from statins anyway. As the extreme form is characterised by LDL receptors working barely at all, even the body going into crisis mode, and trying to take LDL from the blood stream with increased LDL receptor activity, will not work if the LDL receptors are not working sufficiently. Hence the LDL will stay in the blood stream with an extreme sufferer of FH and yet the statin has reduced what little chance the FH sufferer’s body had of making cholesterol within the cell.
There’s a great message on p304 of the book where the Yosephs suggest a notice that should be put up in washrooms:
Employees must wash hands before returning to work.
And do not touch the mevalonate pathway!



Dear Zoe
I have read several of Dr Kendrick’s books and others on the same theme. Also looked at your site and become almost convinced of the “anti statin” ideas and the absense of evidence for a link between eating saturated fats and CVD. I like what I read and always prefer to work things out for myself where possible. So all this is music to my ears.
Both my wife and I are in our mid 70s and were prescribed 20mg statin, in my case about 2 years ago for no reason other than my cholesterol reading was deemed ”too high’ (at about 5.5 I think). Neither of us has heart disease nor is there any in the family. Neither of us is aware of any side effects caused by statins. I have stopped taking them on the strength of all that I have read. My wife remains unconvinced but has a more complicated medical background. We both take regular gym exercise, are non-stressed, not overweight and eat a proper real food diet, including plenty of sat fat from dairy, meat, fish etc. We don’t drink to excess but do like our home made bread!
However my point is this: there is masses of anti-cholesterol info out there on sites like the British Heart Foundation, HeartUK.org, NHS, etc with links to scientific trials that purport to show unequivocal links between high LDL, CVD and stroke. THINCS might call this propaganda or simply ‘out of date’. But is it? Scientific abstracts are notoriously hard to read, let alone comprehensible to most people. I could take all this up with my (part time!) GP but I know what he would say: “come off statins if you like but it’s your risk – beware of the conspiracy theorists (ie THINCS) – don’t believe the internet stuff, etc etc”.
It really is tough. I doubt my ability to challenge him effectively while sitting in the surgery.
I have been on Cholesterol medication for more than 15 years for high Cholesterol. I have been to a clinic for depression and stress and got lots of medication. Has stopped all medication as I could feel that it had side affects which I did not like. The medication did not work well on my brain and it actually made me shake quite extensively. I am still on anti-depressant meds and one sleeping tabled to cope. I have noticed that I am now battling with cramps in my legs, also feel tired with low energy levels, lost some focus brain wise as well as eye wise (vision) and mind not as clear as it used to be, and swollen feet. I went for all sort of tests to determine the cause for the feet problem but the problem persist. Blood flow was checked and all good to go. Could my symptoms be as a result of the Cholesterol medication. Whenever I go for a blood test the cholesterol levels seems on the mark and good to go. What’s your recommendation.
Hi Peter
I’m so sorry but I can’t recommend anything – I can share information and opinions but not advice. That’s for you and your doctor(s).
I’m really sorry to read what you’ve been through and even more sorry because – in my opinion – all of this was avoidable. Everything you’ve described can fall under side effects of statins. Even the low mood which then leads to anti-depressants and then the subsequent problems with those. So yes, in answer to your question – could your symptoms be a result of cholesterol meds? Yes – any patient leaflet will confirm that side effects can include muscles aches, joint pain, leg cramps etc. The Patient leaflet doesn’t list cognitive impairment but forums will confirm this is well known to some people who take statins. Books such as “Lipitor – thief of memory” share what can happen to minds and mood.
I feel so sorry for you. I feel like you’ve lost 15 years of your life and all because cholesterol has become a target per se and not your overall health. The doctors need to be helping your overall health in my humble opinion.
I wish you all the best – Zoe
I am so distressed I need to ask this. In UK, can I find a heart doctor who will take my Dad off dangerous meds and prescribe (relatively) safe natural alternatives? E.G. Hawthorn in capsule form, lowers colesterol and strengthens heart muscles etc without known side effects of statins. My Dad is suffering quite severe memory loss, he is on a high dose 80mg. Soon his quality of life won’t be worth it for the sake of avoiding further heart attack. He is slim, walks every day, and has a great diet .. He came off them for two weeks and improved dramtically, but the Gp got in touch with the heart doc who did his stent op, who said he needs to go back on the statin. I was devastated. I think also it’s the combination of statin, beta blockers and aspirin which is damaging. What do I do? Desperate to find a different way to handle his health that rest of family will go along with, or have confidence in. Looking for heart docs is how I find this page.
Hi Lyn
The Public Health Collaboration keeps a list of health practitioners (I think there are docs, nurses, dieticians etc) who are keen to explore all options – not just meds. I hope this might help
https://phcuk.org/map/
Best wishes – Zoe
My Dr wants to put me on statins, what arguments can I use to make her see they’re not right for me?
I’ve been strict Keto for 10 weeks and my cholesterol has gone to 10.2, some one has mentioned that my body is still healing and that the cholesterol is high in my blood as it’s cleansing the veins and arteries. Also my blood sugar has gone up even though I’ve been <15g carbs per day during my Keto Journey. And of dropped weight from 14st 4lb to 13st.
Hi Ian
I’m not sure if you’re active, but you may find these interesting:
https://cholesterolcode.com/are-you-a-lean-mass-hyper-responder/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6173254/
There is a phenomenon of a hyper responder – cholesterol goes up on a very low car/keto diet. It has typically been observed in athletic/lean types – you might be heading to lean with your weight loss!
The blood glucose is puzzling – this may be of interest here: https://www.dietdoctor.com/low-carb/fasting-blood-glucose-higher
My main post on cholesterol and statins is here: https://www.zoeharcombe.com/2015/03/worried-about-cholesterol-andor-statins/
10 weeks is not long after such a dramatic diet change and weight loss. I would be giving it more time (as a patient and doc) to see where/how things settle down.
Best wishes – Zoe
Zoe, do you know if the authors of the following article received “personal gains” from attaching their names to the piece of garbage?
Lancet. 2016 Nov 19;388(10059):2532-2561. doi: 10.1016/S0140-6736(16)31357-5. Epub 2016 Sep 8.
Interpretation of the evidence for the efficacy and safety of statin therapy
Knowing how statins work, I am astounded that such an article still shows up, even in 2016. I am assuming that this is BIG MONEY at work. I assume you have responded to this somewhere in the past and can direct me to that place. Thanks.
Hi, I have FH, female, age 62, good heart perfusion but cardiovascular symptoms. These are greatly reduced by an anti inflammatory diet. I use supplements, including some cholesterol lowering ones, which reduce it a bit, but since I am not convinced by the model that says lowering cholesterol is what I need to do anyway, not sure if they are helpful. Totally torn between a) ‘irrefutable evidence’ that taking statins will increase my life expectancy and that I am self sabotaging if I don’t take them, and b) all the things I have read to the contrary, and that if statins do help, it is not by their cholesterol reducing ability. My question is what to do for optimum quality of life? Thank you.
Hi
I would like to know what different options Do we have for high LDL-C, LDL-P, etc ? I am 90 % vegeterian, I only consume Omega 3 and twice a week fish, my cholesterol, numbers are high in particular my LDL-P . I spent a lot of money in functional doctors, by the way I am Apoe3/4, thin BMI=20 and exercise everyday and at the end they said the only way to low your risk is taking Red yeast Rice from a good source so my question is What Do I have to do? if I can do something.
Thank you
Richard
Hi Richard
I’m the wrong person to ask because I think you’d be better off not even knowing what your cholesterol is!
Here’s more reading: https://www.zoeharcombe.com/2015/03/worried-about-cholesterol-andor-statins/
Best wishes – Zoe
If I’m reading correctly statins prevent cell pathways for reproduction and cells die. Some cells live longer than others before dividing but how come people are living so long on statins. Do station dosages not get to every cell of do cells find ways around these blocked oathways.
Hello,
I have been diagnosed with FH since I was about 12 years old. My doctors wanted me statins right away, but my doctors and parents agreed to wait until I turned 18. I’ve been taking 20 mg of Lipitor for the past ten years (I’m 28 now) with total levels around 240, HDL around 40, non HDL 200 and triglycerides under 90. Personally, I’m not sure I should be on them even with FH. The more research I do, the more confusing it seems.
I used to be extremely active (marathon running, healthy eating, etc.), but I am finding my muscles to be in too much pain since about a year ago and I find exercising really aggravates my muscles (all over my body, legs, back, shoulders, chest). Now I can only do light workouts and less frequently. I’m not sure why a man my age would have so many aches and pains, but I’m thinking to quit the drug. The pain isn’t enough to stop me from working and being a normal person, but enough to make me uncomfortable most of the time.
My thinking is if I exercise, that would be enough to protect my heart, but my physician seems to think otherwise. Am I crazy? I would like to think I’m otherwise a healthy guy, but it really bothers me. Any advice would be amazing! Sorry for my life story.
Hi Mike
I’m sorry to hear this. I assume you had a genetic test for chromosome 19? Not just ‘diagnosed’ with family history and/or your cholesterol level?
I can’t give advice, but you may find this post interesting https://www.zoeharcombe.com/2016/11/familial-hypercholesterolemia-fh/
and this is my main post on cholesterol and statins https://www.zoeharcombe.com/2015/03/worried-about-cholesterol-andor-statins/
All the best with your research/working out what is best for you.
Best wishes – Zoe
Hi. I was wondering how you felt about Red Yeast Rice.
Thanks.
Not a lot! What’s wrong with leaving cholesterol alone?! https://www.zoeharcombe.com/2015/03/worried-about-cholesterol-andor-statins/
Best wishes – Zoe
Could having taken statins begin the Parkinsons syndrome? Husband just diagnosed, took statins for years. We’re on ketogenic diet (me for 10 years, husband about 8 or 9 years). I feel great, never agreed to take any prescription for “syndrome X”. I’m 73, am thin, strong, energetic, feel better than when I was 20.
Hi Ghost
Given that 25% of the body’s cholesterol is found in the brain (presumably for good reason), it would make sense that statins can ‘begin’ Parkinsons. This link may be of interest.
http://www.medscape.com/viewarticle/870996?
There have been previous claims that statins can help Parkinsons. Dr Uffe Ravnskov suggests the mechanism for this (and similar claims that statins help cancer) is that cholesterol is protective against many conditions. People with high cholesterol are thus better protected against cancer (and Parkinsons). However, people with high cholesterol are more likely to be put on statins. This can produce an association between lower incidents of cancer/Parkinsons and being on statins. Hope that made sense to you – it did to me!
Congrats on your well-being – sounds great!
Best wishes – Zoe
Dear Zoe,
I am 42 years old and have been taking statins for about 8 years. I have inherited high cholesterol from my fathers side. It was about 400 when I was tested. The medicine reduces my cholesterol to about 260. Would I be better off without statins ? My father died of a heart attack aged 56. He was a heavy smoker though.
I don’t know what I should do.
Best regards
Annelise
Hi Annelise
I’m sorry that your father died so young – I think that you’re right to note the smoking – that’s a massive factor, which could make your experience and health very different (plus men are more prone to heart disease than women).
I can’t advise anyone on what they should do. I just research and provide information and views on what I find.
You may find these interesting:
– https://www.zoeharcombe.com/2016/11/familial-hypercholesterolemia-fh/
– https://www.zoeharcombe.com/2015/03/worried-about-cholesterol-andor-statins/
Best wishes – Zoe
I have been diagnosed with FH, and am feeling a little confused. Everything I read on here is against statins (and that is my gut reaction too). However, the section of this article on FH seems to say only that statins would be useless for the people with the most severe form. The conclusion says that statins were originally created for people with FH. Does that then imply that for people with the ‘milder’ form of FH statins are recommended? My total cholesterol reading is 9.2, and apparently rising. My brother has been on statins for years.
Hi Amanda
I don’t know if this post helps? https://www.zoeharcombe.com/2015/03/worried-about-cholesterol-andor-statins/
My personal view is that statins are unfit for human consumption. That’s my opinion and there’s a lot of information in that link that shows why I think that – error of the test not least – yours could be 20% out according to the Fraser paper linked to. It is for each person to read and make their own decision and I admire you for investigating, rather than blindly accepting drugs.
Good luck with your research
Best wishes – Zoe
Hi Zoe,
I bounced into my doctor’s office today for my blood results, proud to show off my slimmer self and all set to explain why my total cholesterol may be higher, but my LDLs lower. In truth, I was looking forward to seeing my fasting insulin and glucose levels and really wasn’t the least bit concerned about cholesterol. And I was going to boast about my new low-car/ketogenic way of life and had a list of recommendations for her to check out about cholesterol, fat and insulin. My doctor has been prescribing statins to me since I’ve known her and I haven’t the heart to tell her I never take them. So I am always lying when my bloods come back and my normal levels are still around 7.5 mmol/l. She freaks. But today she more than just freaked and I drove home with her words ringing in my ears: ” I have never seen levels so high! You are heading for a heart attack! Here is a referral to a cardiologist who you must see asap!”
My total cholesterol has hit 14 mmol/l and that IS high, isn’t it? Yet I don’t have any of the symptoms of FH although my mother has high cholesterol and all four of us seem to have inherited it. I don’t smoke, my BP is normal, I am stronger than just about every other 58 year-old woman I know and I feel fantastic, especially since going to war against carbs. I get told I look 10 years younger because my dermal layers are firm and supple! My fasting insulin is 7 and I am 56 kgs, down from 64, and heading for stability around 53 at this stage. I realise I was/am a sugar addict with insulin resistance but for the past 3 months I have become keto-adapted, and follow, more or less, a ketogenic 16:8 diet. My inflammatory markers are normal, so for all intents and purposes I am more healthy than unhealthy except for these blasted LDLs.
Should I be panicking about dropping dead? I don’t want to take the new statin, Atorvastatin. I am about to order “How statins really lower cholesterol…”. You, Jason Fung and Ted Naiman are my cyber-mentors and I trust you 100%. I think I may just fall in that 1 – 2% of people whose lipids don’t respond well to a lchf diet ( quoting Andreas Eenfeldt ). Do you have any advice?
Hi Supatra
This post might help https://www.zoeharcombe.com/2015/03/worried-about-cholesterol-andor-statins/
14 is high – if your normal levels are 7.5 – my first thought would be that there’s an error with this reading. One of the links in the “Worried about” post above goes to a Fraser BMJ article where errors of 20% are shown to be normal! It could be an error like this or a complete mess-up error – they do happen!
My second thought would be – even if your levels are in double figures, if they are normally around 7.5 – is anything going on in your life? You feel great and the details you share do paint a picture of a happy, vibrant person excited about her current health but the body makes cholesterol for a reason. Are you stressed? Injured? could you be fighting an infection? Have you not been near the sun for a long time?
Another of the links from the “worried about” will take you to graphs where – for 192 countries – the higher the cholesterol, the lower the death rate (heart and all causes) – especially strong in women. The cardiologist probably won’t believe it despite the fact they could draw the same graphs from the same WHO data in the couple of hours it took me.
My expectation is that you will be under more pressure from the cardiologist to go on statins. That’s why my worried about post laments that we ever get this waxy substance measured in the first place! You’re now in the system – good luck!
Best wishes – Zoe
p.s. another terrific book is Dr Malc Kendrick The great Cholesterol Con
I have been horrified by the revelations in Zoe’s article and also in this thread. About 20 months ago my doc suggested that I start to take a statin axs ‘the guidelines’ had changed and I now fell within the target group. I was diagnosed in 2014 with Paroysmal Arial Fibrillation – a relatively common heart rhythm disorder treated by beta blackers and when I hit 65 next year, by a blood thinner, to prevent stroke. So, as advised, I started on Lipitor 10 mg – which I took for about 12 months. two blood tests in that time with nothing looking amiss. Then at the next visit, was informed that I needed to take 20mg as my cholesterol needed to come down (was under five to begin with). SO I took 20mg as directed – started to get bad leg and foot cramps, plus a few tummy pains, but lived with it. Then about three months ago, the doc informed me that my triglycerides, at 3.0 were double what they should be. So the dose went up to 40mg the cramps got worse and spread to my hands, I put on 4lb in weight, which all felt like it was just below my ribs, was tired a lot more and started getting headaches when I woke. At the first routine blood test last week, the result showed that my liver enzymes were elevated – I asked what happens now and my doc said that it was hard to know what to do. We agreed to reduce the dosage by 10mg and test again in four weeks. In the meantime I did some reading on the internet and was horrified. I decided that I shall never take statins again, so I stopped them. Just over a week ago…now I feel as ill as I have ever felt. An avalanche of symptoms ranging from constant nausea to complete exhaustion, metallic taste, pains below ribs, in abdomen, bloating, dizziness, tearfulnes, chills, headaches, waking through the night. On the third night after I stopped I was up and down all night retching, feeling violently sick, running to the toilet, chills and shaking. Now nearly a week later I am utterly wiped out, no energy whatsoever, nauseous, no appetite at all, dry mouth, no interest in food…etc. I dragged myself to the doc this morning and his view was the there was an event – me stopping statins, and now this. Too much of a coincidence to dismiss – “give it time to play out”. I asked him directly had he encountered other people who felt so ill coming off of statins – his reply – “everyone is different”. This was not my usual doc however If I am not better in three weeks, I have to return for a full blood count. Please does anyone who has experienced statin withdrawal have any suggestions… i feel as though I am inhabiting someone else’s body since I stopped the statin a week ago. Jus feel so ill and exhausted. Have cancelled my holiday next week – just can’t imagine going away feeling like this.
Hi Marion
I’m so sorry to hear you’ve been a victim of the statin profit lovers. I have not heard of withdrawal symptoms before – I have heard people saying they felt almost immediately better stopping statins and some people sadly did not regain the muscle/mind function they had before statins. Have you tried googling for forums of ex statin takers? It would be unlikely that you are alone
For interest for others reading this horror story, this is the patient leaflet for Liptor https://www.medicines.org.uk/emc/PIL.2498.latest.pdf
Check out common side effects about the liver p4 – and a few concerns expressed about the liver throughout!
And your cholesterol was low (realtive to the genuine average) to start with
And statins might buy a couple of days if you’re lucky (and not by lowering cholesterol) http://bmjopen.bmj.com/content/5/9/e007118.abstract
And they don’t help women
And, and, and
Time to sue some people in my opinion!
Best wishes – Zoe
Pingback: Cholesterol – is it the baddy we’ve been taught to believe? | Karen Mazzella
In UK in 2001 I had a heart attack at the gym caused by over exercising, my cholesterol was checked at 4.5 and I was put on Simvastatin 40mg. Through diet & moderate exercise on my first year med exam I cut it down to 2.4 and was told that was too extreme. Every doctor has always told me to keep taking meds. Last year in Dominica W.I. I was diagnosed as having calcified plaque in arteries of both legs. I was told keep taking the meds and speed walk which helped but I have bad cramp in the legs. tonic water/quinine has helped but the walking is very difficult now. Also having problems with eye strain and sleeping. I am approaching 70 in November and at present while awaiting a US visa in Haiti where I would not use the medical services if possible. Any advice will be considered gratefully
Hi George
I’m not surprised you’re experiencing leg cramp/difficulty walking/eye problems/sleep problems – these are all classic symptoms of statins.
This may be of interest: https://www.zoeharcombe.com/2015/03/worried-about-cholesterol-andor-statins/
Your cholesterol at 4.5 was absurdly low (in my opinion – and relative to the average person). At 2.4 I’m surprised you were still functioning at all!
You may also be interested to know that even the patient leaflet cautions against anyone over 70 taking statins – because it is well known that higher cholesterol is better when older.
The graphs here confirm that higher cholesterol is better when 192 countries in the world are reviewed together – by someone not funded by statin makers (me!) https://www.zoeharcombe.com/2010/11/cholesterol-heart-disease-there-is-a-relationship-but-its-not-what-you-think/
I can’t advise you – but do see this as your choice and don’t be bullied by white coats who don’t have to suffer the pain and disability that you are experiencing. I know I personally will never let a statin pass my lips – easy call for me!
Best wishes – Zoe
Zoe, I am in America and hear the same advice all of the time. My own family is pressuring me to take statins – even today when news of a co-worker having a heart attack hit close to home. My cholesterol numbers were 271 total, 45HDL, 187 LDL. My Triglycerides were 194, and Fasting Blood Sugar Level was reported as 104. All figures are using mg/dl. I have high blood pressure (runs in family as does high cholesterol) that I am taking Lisinopril. My GP has been suggesting statins for some time now as well. Suggestions?
Hi Robert
I get asked about cholesterol so often, I wrote this post to signpost to other interesting articles https://www.zoeharcombe.com/2015/03/worried-about-cholesterol-andor-statins/
Hope it helps
Best wishes – Zoe
Hello Zoe.
How I’ve missed this website I cannot understand with all the research I’ve done, still, today, here you are. I am an American living in England so we’re in mmol/l rather than mg/dl but I can translate.
My father died of a massive heart attack at age 57 – my age now. Turning 57 scared me witless because I learned at age 50 of my high cholesterol and a few years ago I did a family tree on my father’s side and it turns out quite a few of them died of strokes and heart attacks and sometimes both. One of my past family sets married and they both died of heart attacks. Doesn’t bode well…
Anyway, my cholesterol at 50 was 12.5 (that’s 483 roughly). I was immediately put on Simvastatin 40’s I think, which I realised fairly soon I didn’t get on with. Over the past seven years I have tried several different statins, ending with Crestor (because it’s water soluble instead of fat soluble) and have been given Ezetimibe but I have had so much trouble with statins that I really don’t know if I can try another type of drug. I have had a check and my arteries are clear but my carotid arteries are over 50% blocked. I did some research and got serrapeptase for that which I take when I get up in the night for a pee, as it needs to be taken on an empty stomach.
I suffer with tinnitus, which I reckon is something to do with this, actually when I took Crestor, that subsided a bit. I also have this sort of thudding which happens a bit like a whole body pulse. I reckon all the symptoms are to do with the carotid, I think they call it a carotid bruit. I notice when I drink alcohol, it gets worse.
Basically, I’ve got a problem and I am told it’s cholesterol but I’ve read all the books and now you’re saying the same thing and I don’t trust pharma anyway. I work in a pharmacy and I think half the people on more than ten drugs a month are probably fighting off side effects from drugs by treating them with drugs. I am a true skeptic.
I went to a specialist but he was all about drugs too. All I want is to know the best way to alter my lifestyle and still have a life, have the odd glass of wine, eat some chocolate sometimes (dark, of course!).
I have increased my daily exercise by buying a good quality rebounder (Bellicon) and just got a smoothie maker so I can change the way I snack and do breakfast. I take magnesium, vit C, glucosamine with chondroitin (for arthritis), garlic, fish oil, vit D (because England is rarely sunny). I would like to know more about diet for FH, if that makes any difference.
Is there anything else I can do? What about Omacor? Do you know of it? The FH thing is a pain because there is a lot of research done on cholesterol but the FH issue gets mentioned rarely, so I want to thank you very much for addressing this.
Hi Cathy
I’m so sorry to hear about your family losses so young.
This post may help: https://www.zoeharcombe.com/2015/03/worried-about-cholesterol-andor-statins/
Check out the video at the end (Dr Malcolm Kendrick) – about 15 mins in he asks the FH question the right way round. You may also like to get hold of Dr Uffe Ravnskov Ignore the Awkward – covers FH often -esp. chapter 3. The issue isn’t cholesterol and lowering it won’t help – that’s our view and that of many who have nothing to gain from pharma zillions.
Not sure there is a diet for FH – the best diet (in my view) is always real food based (meat, eggs and dairy from pasture living animals; fish; vegetables). Depending on weight, fruit in season, nuts and seeds can also be enjoyed – as can red wine/dark chocolate and some non-wheat grains (oats/quinoa/rice) by many people. What no-one needs is sucrose/white flour/processed vegetable oils.
You can see from this blog and the “worried about” one – I think high LDL is a symptom of FH, not the problem with FH. The problem is that cholesterol is not getting to the cells where it is needed – heart cells included. Keep reading!
Best wishes – Zoe
Thank you, Zoe, I appreciate that. I had an appointment with my GP just today and he has now prescribed me Omacor 1000mg twice a day (it’s omega-3 acid ethyl esters). I suppose it’s worth a try but I will keep with good food and exercise. I do eat normal food, I eat butter, meat, vegetables, nuts, seeds and although I can’t really use milk, I do eat cheese and I use soya milk.
I try to avoid white flour and processed oils at all costs. I understand that oxidation has something to do with it all, and I try to use the right oils for the right temperatures, keep the sweet things to a minimum, except for fruit. I’ve learned to make coleswaw with yoghurt and only a little mayo, but the mayo I use is made with cold pressed rapeseed oil. It’s quite filling as I use lots of veg and apple with it, so I often use it as a snack when I’m peckish.
I appreciate the information you’ve provided, I will keep on reading, and will keep this site bookmarked, as amazingly, I’ve actually never noticed it before. Well done for this page, you’ve probably made a lot of people feel better about not taking statins. I simply cannot take them, they make me ill. When my GP sent me to a specialist, I thought, great, let’s get our information and maybe tests to see how things are, then a dietitian perhaps, or tips and hints, etc, but no… to my problem of not tolerating statins, he responded with… yet another statin. Arrrghhh!
At the end of the day, as far as life expectancy is concerned, the best you can do is enjoy what you are given; I never want to live to be over 90 anyway, who wants to end up in a home? Certainly not me! I try to enjoy each day and keep a good mental attitude, and enjoy what there is to enjoy, suffer what there is to suffer, life is a rich tapestry of all these things and everything in between, it’s for our learning, and you are doing a good thing helping people do that, and it’s very much appreciated.
In the meantime, I’ll keep my eyes peeled for that magic potion that makes the cholesterol do its job properly for those of us with FH!
Thanks again, you’re doing great things.
All the best
Cathy
Great post. Sad though for those of us with FH. The basic idea as I read it is:
Have FH?, tough luck! Statins not going to help, nothing else going to help either, and pharma sure as hell isn’t looking to find a solution. You’ll probably die from CVD before your hair starts turning grey and there is not a thing you can do about it.
Hi Rob
I don’t think it’s that bleak – check out Dr Uffe Ravnskov’s work Ignore the Awkward – Chapter 3 especially (it’s on open view somewhere but I can’t remember where – sorry!) He looked at the life expectancy for those with FH and found it to be little different to those without – higher risk of some things, lower risk of others.
Check out this video (c. 15 mins in) where Dr Malcolm Kendrick asks the FH question the right way round https://www.youtube.com/watch?v=8ls9HWRxvMo
Best wishes – Zoe
Hi Zoe, Many thanks for taking the time to explain all this as it’s hard to find real evidence and easy to read articles like this. I have FH (diagnosed age 13) and would desperately like to know if I should carry on taking my 40mg of Atorvastatin which I’ve been on for over 15yrs (well, Simvastatin 40/80mg for many of those years). Is this drug still for someone like me or should I come off it, this is the question? I am nearly 40 this year, pre-menopausal, my stats vary from 6-10.7. My father had FH and died of a heart attack aged 62. His father died before the age of 40. My siblings have all inherited it to some degree and my brother has had heart complaints. I have a terrible memory and can perhaps put it down to statins as it used to be great. I have bad gut issues and was also diagnosed with an underactive thyroid over 10yrs ago and finally tested for Hashimoto’s last year and found that I had that particular disease as well. I cannot determine if I should be on these pills and am scared about what they are doing to people and which is the worse evil, statins or FH??? I would REALLY appreciate a response and an answer would be so fantastic!
Hi Abigail
I sadly can’t advise you on this. I can only share information and pointers to things of interest. This is the ‘signpost’ blog to the key things I’ve written about cholesterol and statins (https://www.zoeharcombe.com/2015/03/worried-about-cholesterol-andor-statins/)
The video mentioned, just above “more reading” is highly recommended – I think it’s about 15 mins in that Dr Malcolm asks the FH question the way it should be asked – watch the whole 30 mins if you have time – genius! Added to the further reading, you may like Dr Duane Graveline’s books (Statin damage crisis and Lipitor – thief of memory) – he has personal experience of some of the memory problems you mention.
Personally, a statin will never pass my lips. I would not worry about cholesterol. I would worry deeply about taking statins – not lease because of what’s in this post that you commented on. But that’s me – you’re doing the right thing reading and seeing what you think about the topic.
I presume you never want children? You can’t have a baby while on statins – babies need cholesterol to be formed, let alone healthy. So do adults, but there I go again!
Best wishes – Zoe
I have stopped taking the Statin drug Lipitor for six month.I take two drugs presently LISINOPRIL-HCTZ 20/25 plus a THYROID DRUG 75MCG daily. Six month ago I was paying a lot for medications I did not need. I read your mail on the Internet today and believe that I am on the right track since I feel good and can do without the nasty side effects. Thanks Karl
I am also hypothyroid and took Lipitor / Atorvastatin for the second half of last year.
It may have been due to my condition or another drug, but initially I felt I might have MS, with loss of executive function.
Aches in wrist and hip joints (along with reading pages such as this) prompted me to cease taking the statin. I had headaches initially, so the withdrawal should perhaps be tapered.
Increased alertness; easier breathing due to less crusting of nostrils ; eyes less gritty and sore; big reduction in chilly feeling and variation of body temperature are benefits from stopping that I’m aware of.
I’m a 45 year-old female who just had a completely unexpected stroke (no real risk factors). My cholesterol levels were not considered “high” but the cardiologist and neurologist want me automatically on Lipitor in addition to Plavix and baby aspirin. I am also on Levothyroxine for thyroid. I hate being on all of these drugs.
On top of it, they discovered a PFO and want me to get it closed despite knowing if that even contributed to the stroke or lack of data re success of PFO closure for recurrent stroke prevention. (They say better to be safe…)
I feel totally lost. Any advice would be greatly appreciated…
Hi NG
I’m sorry but I can’t offer advice. I’m not a doctor and even a doctor wouldn’t offer advice about this kind of thing without knowing you/your history etc.
This is a sign post article to the key things I’ve written about statins and cholesterol https://www.zoeharcombe.com/2015/03/worried-about-cholesterol-andor-statins/
The only thing I would say is don’t be bullied by white coats – it’s your health, it’s your body. They don’t have to live with side effects – you do.
Good luck!
Best wishes – Zoe
How would you reduce high blood pressure. On meds but would like to come off them. Can you just stop them. Thanks
Hi Bids
Fastest way I know is to go on a low carb diet (under 50g a day) for 2-3 days. This drops glycogen from the body and the body holds 4 parts water for every 1 part glycogen. You can lose c. 1lb (500g) glycogen and 4lb (2kg) of water in a couple of days. This reduces BP immediately. Think of BP in the body as water in a pressure cooker – add more water, the pressure goes up; reduce water it goes down – the body is the same.
Is your BP actually high or what has been reinvented as high? (https://www.zoeharcombe.com/2014/06/diabetes-cholesterol-bp-normal-is-no-longer-normal/)
Normal is 140/90. People with normal are told they are high so that they can be medicated. Don’t be part of the crime!
Best wishes – Zoe
Hi I’ve recently stopped taking artovastatin after about 1year I have had tendon damage and total muscle wastage on my right pectoral muscle also muscle cramps and tingling in my right hand my doctor refuses to see any link to statins and has booked an appointment to have a mri scan saying he believes my problems stem from my spine because my neck is stiff wich has been stiff for 20 years or more just hope he’s right after what I’ve been reading about statin side affects
Maybe half of Congress is on statins, that would explain a lot.
I am 69 years & in good health generally but overweight by 40 lbs. {s/b ~190 lbs}. Been on statins for 12 years & now taking 40 mg simvastatin. Total cholesterol level 2 months ago showed 160. Have read many statin blogs looking for info but my question is are there any serious, health threatening side effects as a result of getting off of statins totally and completely. I would like to to stop taking them. You have a site that presents info in a very comprehensive manner.
thanks
Steve
Hi Steve
An interesting question and I can’t advise – I can only suggest things to read.
Hot off the press you may find these very interesting
http://www.drjoetoday.com/statins-treatment-extends-life-by-four-days/
and the original is here http://bmjopen.bmj.com/content/5/9/e007118.long
This suggests you might lose 3 days! Then weigh that up against all the side effects (listed on the patient leaflet) you’re risking and the understanding from what statins actually do in the body from the blog this comment is attached to.
You may also like to read the patient leaflet for age cautions. I’ve seen 70 as the age beyond which even the patient leaflet cautions. That’s because the evidence for longevity and high cholesterol is particularly strong in older people.
Best wishes – Zoe
Interesting info. So, if someone needs to lower there cholesterol, what is the best procedure?
Hi Karl – you’re asking the wrong question. The right question is WHY would you want to lower cholesterol, not HOW.
https://www.zoeharcombe.com/2015/03/worried-about-cholesterol-andor-statins/
Best wishes – Zoe
I WAS TAKING SINVINS TATIN AND THE DR TOOK ME OFFIT AND PUT ME BACK ON IT BECAUSE HE FELT AS THOUGH I SHOULD BE ON SOMETHING SO I TOOK IT FOR 5 DAYS AND I WS GETTING LEG PAINS HAND PAINS AND NOT FEELING WELL HE TOOK ME OFF IT FOR 6 WEEKS AND I AM GOING TO HAVE BLOOD WORK DONE AGAIN IF THERE IS SOMETHING ELSE I CAN TAKE I WOULD RATHER SO I DON’T HAVE ALL THESE LEG AND JOINT PAINS
Hi Paul
That’s not the right question to ask. The right question is – why would you want to lower your cholesterol?
https://www.zoeharcombe.com/2015/03/worried-about-cholesterol-andor-statins/
Best wishes – Zoe
First,
Wow! I had no idea it was this bad. And this post is from 2013 and nothing has been done? Where is f… media??? (I don’t use that kind of language, but this is a really worthy exception.)
Second,
You write “This book should be read by every person BEFORE they either prescribe or take statins.”
I think we all should give our physicians a copy.
Now I have to get the book and then translate it to my mother…
Thanks for all the work you’re doing to keep us informed!
Holy crap…I read the rest of the article. I’m scared to tears now.
I’m not saying all medical practice is this way, but it seems more and more from the drug companies is about pure profit, not the health of the people they serve.
To think that statins have caused people to commit suicide from cholesterol deprivation and agonizing muscle pain, and they STILL push for these drugs and people still advocate for them!!! They manipulate statistics, refuse to report the severe cases, downplay the horror stories of real people (or as they would call them “patients”), they cripple lives and even take them from us, yet they make a huge profit off of them in the meantime. This should be labeled as organized crime.
They are even trying to CHILDREN on these drugs now, among ever expanding “mental illnesses” aimed at children and adolescents that are just normal, healthy and reasonable behavior. Talking about putting statins in the F**KING WATER SUPPLY?!? If that was a joke, it was an ill suited joke that could be taken seriously someday.
How many more lives will be taken? How many children will report of suicidal thoughts? How many more antidepressant drugs will be prescribed? How badly will that impact their health? They are playing with our lives as though we are toys and bathing in the money those lives give them, not seeming to care about if those lives are crippled or stolen away from them. It seems as though we are the guinea pigs they so enjoy torturing to death, all the while laughing on their way to the bank and back.
This should be criminal. It deserves to be.
My husband had 3 stints put in a year ago. Cardiologist prescribed 80 mg Lipitor, which we thought was over the top considering his blood work showed everything within normal ranges. Dr. said that he wanted to bring my husband’s cholesterol waaaay down because he has so much blockage. Our Internist agreed that he needed statin, but lower to 40mg. Resulting blood tests showed high muscle enzyme, so he changed the statin to 10mg Pravastin. We are very uncomfortable with statins to begin with, but was warned that without the statins he would have a heart attack. My research is leading us to remove the statins completely, but we are afraid to do so. What should be done to optimize heart health. He walks on the tread mill 5 days a week, and drinks organic bullet: apples, beets, carrots, no drinking, no smoking… eats healthy. I would appreciate your advise.
Hi Chris
I’m sorry to hear about your husband and the challenges that both of you are having with treatment.
I can’t give advice – I’m not a doctor and no doctor would give drug advice without meeting/testing someone in person. This will signpost all the key articles I’ve written about cholesterol and statins (https://www.zoeharcombe.com/2015/03/worried-about-cholesterol-andor-statins/) and it suggests further reading.
You may find this interesting on stents (http://drmalcolmkendrick.org/2014/09/12/watch-this-2/)
Why would the human body make cholesterol if it were trying to kill us?! Why is cholesterol lowering a global obsession when every human being would die instantly without cholesterol?!
I sometimes wonder if some docs had their common sense removed at med school!
Good luck with your reading and researching
Best wishes – Zoe
Just FYI, I am intimately aware of a company that did studies on may stents. Guess what? They lied to the FDA. They provided reports in which they removed outliers from the data just before the report was sent to the FDA. They were influenced to do this by the manufacturers, all of whom had people working INSIDE this company that was supposed to be doing “independent” studies of the stents. Just thought we’d all find that amusing. I trust NO doctors, I trust NO goverment agencies. I watched them ALL falsify data and then put these non-studied devices into peoples’ bodies. It’s unbelievable. I sincerely hope everything goes well for you.
So…I have familail hyperchoelsterolemia, or as my mom put it “FATAL familial hypercholesterolemia”…now I’m not so convinced it’s such a fatal thing after all!
I have the strongest immune system in my family. High cholesterol helps with immune function.
I wouldn’t say I “suffer” from FH. I’m grateful that I have it. I read an article that stated mice with FH took 8 times the amount of toxins to kill than those with normal cholesterol levels. 8 F**KING TIMES!!
My LDL was about 250. My doctor wants it to be at 150. I’m not so sure that is a safe number…worse yet, he wants it to get lower as I age. or at least that is what he implied stating “I would be much more worried about it being as high as it is if you were in your 40s or older.” Yet he insists that he takes his patients off of their cholesterol lowering medicines (or red yeast rice, which IS a statin!) “if they get too low”…how low IS “too low”? I’m wondering. Too low could mean “damaging dangerously low level” kind of low.
I got my LDL lowered to around 150…WITHOUT statins OR red yeast rice! Though i would like it to be a bit higher. I did that by eating butter, three to four free range eggs a day, four glasses of raw whole milk a day and even pork rinds. Yes, pork rinds! Those were more so for snacks every three to five days. I got most of fat from the other things though. i did use plant sterols, but I don’t know if those had anything to do with it.
In fact, I had some really bad thoughts while using red yeast rice. I questioned whether I wanted to live, not from muscle pain or the like, but from the panic attacks, mild paranoid hallucinations and sudden aggressive tendencies. Like staring at the kitchen knives thinking “do I really want to live? Is their a less painful way to end it?” kind of bad thoughts. The “oh no! Mom is fighting with my step dad! I had better keep a knife by my bedside in case she tries to do…some kind of horrible things to me!!!” kind of bad thoughts. Creepy as fu…well, you get the point.
Good thing a nightmare gave me a rude awakening, literally! I stopped it and felt better. if my doctor ever says I need statins I will be furious. He has already told me he wants my cholesterol to get LOWER as I get older…after my experiences on red yeast rice? F**k no! It’s sad too. As he is one of the first to actually be willing to talk about natural alternatives and recommending vitamins!!!
Dear Zoe
My wife has suspected FH and of course has been recommended to take statins. This led me to review the evidence, something I have intended to do for some time because I myself have a steady stream of patients who have been put on statins (a few by me, I confess) and who tell me of unacceptable side effects; and I listen to my patients.
The clarity of your research persuades me that neither of us should accept statins, and I shall have to think through my attitude to them professionally with great care (the problem is that I work with colleagues who take a different view, and patients are shared – but I certainly shan’t be initiating Rx with statins). For that I am grateful: thank you.
I have to respond to the criticism that we as doctors should know everything…I accept it in the spirit in which it is given; but you yourself have dealt with a miniscule area of everything we are supposed to “know” – understanding human physiology is beyond any of us and quite incomparable to what a mechanic has to retain (my car is not “fearfully and wonderfully made”!) I see patients every 10 minutes as a UK NHS GP, and I’m afraid as generalists we sometimes just have to take guidance (such as NICE produce) at face value. But I do agree that we also have to investigate with care those areas where our specialists seem to be wanting us to do something which appears to produce negative consequences. In that people like you are such a blessing.
The truth is that, whilst much medicine has brought huge benefit to mankind, tinkering in areas we don’t fully understand whilst ignoring side effects in multiple systems – side effects we also don’t fully understand – doesn’t make sense. We should seek advance through research, but not promote it prematurely for financial gain. And we should present the degree of perceived benefit honestly and simply. And we should avoid poly-pharmacy as much as possible.
I shall continue to raise this issue with colleagues. I am an unimportant and near time-expired cog in a vast wheel, but I might at least precipitate some to think this through.
Kind regards and thank you again.
Hi Michael – thank YOU! For your wonderful note – if only all GPs were as open minded. We sadly get regular horror stories of people who have refused statins or tried them and stopped taking them because the side effects have been so bad. Some docs have been very supportive but others have demanded disclaimers to be signed; patronised; scorned; scoffed; bullied; derided and all sorts. It’s driving people away from surgeries and adversely impacting what should be a treasured doctor-patient relationship. I avoid docs at all costs, don’t go for check ups, screenings etc, because I’ve lost respect for the continual lowering of targets and concomitant over-medicating (https://www.zoeharcombe.com/2014/06/diabetes-cholesterol-bp-normal-is-no-longer-normal/) I’m better off left alone!
Dr Uffe Ravnskov has written some great stuff on FH. It’s a genetic defect and genetic defects generally are not good news, but the high cholesterol is a marker of a problem (the LDL receptor not working) – not the problem itself. Uffe has shown that FH people die less of other conditions and they die slightly more of CHD in younger years. An FH person in their 40s? 50s? I’m not sure of the exact age beyond which one has ‘survived’ the worst period, lives as long, if not longer, than a non FH person. And statins won’t help – they’ll just impair the cells from making the cholesterol that they need and that they can’t get from low density lipoproteins because they can’t receive the LDLs into each cell!
Other great reading is Dr Malcolm Kendrick’s The Great Cholesterol Con – brilliantly informative and one of the funniest books I’ve read.
Good luck to you and Mrs H!
Best wishes – Zoe
p.s. I do say in my 2010 obesity book that the GP is a marvel for the breadth that they must deal with – a broken bone one minute, cancer diagnosis the next, an infection, depression – it is quite incredible. I guess – even more why I get upset that the respect that GPs deserve is being undermined by NICE non-independent (https://www.zoeharcombe.com/2014/07/nice-has-ended-any-debate-about-its-independence/) guidelines to move ‘normal’ goalposts and to medicate everyone! Dr Aseem Malhotra is doing some brilliant work in this area too (https://www.zoeharcombe.com/2014/06/doctors-tell-nice-youre-not-independent-youre-not-evidence-based/)