
Cholesterol & heart disease – there is a relationship, but it’s not what you think
This post is dedicated to Anne who asked me a great question about cholesterol. It made me do what I had been meaning to do ever since I read Dr Malcolm Kendrick’s The Great Cholesterol Con…
Dr MK ran some analysis on World Health Organisation (WHO) data. The WHO has extensive data from almost 200 countries on more health measures than you could imagine – definitely worth a look one rainy, wintry afternoon. This is where Dr MK presented the world with two different Seven Country Studies – (for those of you who aren’t familiar with the history, it was the Ancel Keys’ Seven Countries Study that started all the fat heart hypothesis stuff). Dr MK took the seven countries with the lowest saturated fat intake and then the seven countries with the highest saturated fat intake. You may need to read this twice – but he found: “Every single one of the seven countries with the lowest saturated fat consumption has significantly higher rates of heart disease than every single one of the countries with the highest saturated fat consumption.”
The next chapter in The Great Cholesterol Con goes on to look at cholesterol and heart disease (and overall death rates) and quotes many great studies where it is shown that lower cholesterol is associated with higher mortality. However, it did leave me thinking – having run the data on saturated fat and heart disease, let’s just run all the data on the cholesterol and heart disease and get to the bottom of this hypothesis from all parts of the allegations.
It actually didn’t take that long – less than a couple of hours one Saturday afternoon. You go to the WHO statistics area of their web site and then pick data for cholesterol from risk factors (how judgemental to start with!) and then look under: Global burden of disease (mortality); All causes; Non communicable diseases and then G Cardiovascular disease (shortened to CVD). CVD deaths include ischemic heart disease and cerebrovascular disease – that means fatal heart attacks and fatal strokes to us. You find the most recent year where you can get both sets of data to compare like with like. This turns out to be 2002. You download their very user friendly spreadsheet data (CSV) – cut and paste it into an excel file and then try to remember how the heck to do scatter diagrams in excel!
Before telling you the results, we need to go back for a quick reminder on what we know about cholesterol and then hopefully this can serve as a factsheet for all the cholesterol questions we continually get.
The role of cholesterol
It is virtually impossible to explain how vital cholesterol is to the human body. If you had no cholesterol in your body you would be dead. Every single cell of your body is covered by a membrane (think of a membrane as the ‘skin’ or protective barrier around each cell). This membrane is made largely of cholesterol, fat and protein. Membranes are porous structures, not solid walls, letting nutrients and hormones in while keeping waste and toxins out. If cholesterol were removed from cell membranes they would literally explode from their internal water pressure. Human beings quite simply die without cholesterol.
Cholesterol is vital for hormone production – the sex hormones and therefore the entire human reproductive system are totally dependent on cholesterol. Hence, not only would humans die without cholesterol, the human race would die out.
Cholesterol is vital for digestion. The human body uses cholesterol to synthesise bile acids. Without cholesterol-rich, bile salts, the human body could not absorb essential fatty acids or the fat soluble vitamins (A, D, E and K) and serious, even life threatening, deficiencies could develop. (It is interesting, therefore, that nature puts cholesterol in virtually every food that contains fat – providing a digestion mechanism in tandem).
Cholesterol is vital for the brain, central nervous system and memory functions (hence how the side effects of statins include memory loss, mental confusion and people generally just not feeling themselves). Even though the brain is only 2% of the body’s weight, it contains approximately 25% of the body’s cholesterol. The vital connections between nerve endings in the brain, which help to conduct the electrical impulses that make movement, sensation, thinking, learning, and remembering possible, are largely made up of cholesterol.
Cholesterol is critical for bones and for all the roles performed by vitamin D. Vitamin D is best known for its role in calcium and phosphorus metabolism, and thus bone health, but we are continually learning more about potential additional health benefits of vitamin D from mental health to immune health. Vitamin D can be ingested (and is, interestingly again, found in foods high in cholesterol) and it can be made from skin cholesterol. Modern ‘health’ advice to avoid the sun, take cholesterol-lowering drugs, eat a low cholesterol diet (whatever the heck that is supposed to be) – combined with there not even being a recommended dietary allowance for vitamin D – is undoubtedly contributing to avoidable modern illness.
One of the key reasons that we need to spend approximately one third of our lives sleeping is to give the body time to produce cholesterol, repair cells and perform other essential maintenance.
This gives you the headlines of the vital functions that cholesterol performs, but hang on to that bottom line – it is utterly vital and we die instantly without it.
You may be familiar with the term essential fatty acids or essential amino acids (proteins break down into amino acids). The term ‘essential’ used like this in nutrition means that it is essential that we consume it in our diet because the body can’t make it. The body makes cholesterol. That says to me that cholesterol is even more vital than essential fatty acids or essential amino acids – even though these too are life critical – and therefore the design of the human body is such that it was not left to chance that we needed to get cholesterol from food. Of the 500 or so roles that the liver has – one is to produce cholesterol. It is too vital to be left to chance.
What went wrong?
So, how did something so life vital become more vilified than a mass murderer? I think it comes down to three things (and I don’t take credit for this view – it is there to be worked out by anyone who traces back the history and Kendrick, Uffe Ravnskov and all the thincs.org guys have led the way):
1) Rabbits;
2) Ancel Keys;
3) Money!
1) In 1913, a Russian chap called Nikolai Anitschkow decided to feed rabbits purified cholesterol and he managed to get their blood cholesterol levels in excess of 1,000 mg/dl (nearly 26 mmol/L! Most UK people have levels of 5-7 mmol/L). He then noticed the formation of “vascular lesions closely resembling those of human atherosclerosis” forming in the arteries of the rabbits. The obvious flaw in the experiment should have been that rabbits are strict herbivores. They do not eat animal products, which is the only source of cholesterol. Hence rabbits are in no way designed to digest cholesterol or animal fat and no one should be surprised if cholesterol or animal fat ended up stuck in any part of the poor rabbit. The only surprise is that no one thought to ask Anitschkow why he was feeding cholesterol and animal fat to herbivores. Interestingly, far less well known is that a parallel test was done on rats and dogs (omnivores) and feeding cholesterol to these species failed to produce lesions.
2) Ancel Keys. Remember the Minnesota experiment that I so often refer to? A brilliant and unbiased piece of research, which has given the world one of the best insights into low calorie dieting ever done – it was pure genius. This study made Ancel Keys the man of the moment and I guess he wanted to follow it with something equally impactful. There is an anecdote in The Great Cholesterol Con and on p113 of The Obesity Epidemic where Henry Blackburn, one of Keys’ closest colleagues, tries to explain what may have fuelled Keys drive to find a connection between diet and heart disease.
What is little known is that Keys originally tried to establish a link between cholesterol in food and cholesterol in the blood (our cholesterol levels when we have a blood test) because he thought (probably because of poor Bugs Bunny) that cholesterol in the blood causes heart disease.
Keys did multiples of studies, changing the diets of his human ‘guinea pigs’, and he presented his conclusions in The Journal of Nutrition, November 1955: “It is concluded that in adult men the serum cholesterol level is essentially independent of the cholesterol intake over the whole range of natural human diets. It is probable that infants, children and women are similar.” i.e. I only tested adult men and there is no relationship between cholesterol eaten and cholesterol in the blood and it is probable that there will similarly be no relationship for women or children.
In 1997 Keys put this even more assertively: “There’s no connection whatsoever between cholesterol in food and cholesterol in blood. And we’ve known that all along. Cholesterol in the diet doesn’t matter at all unless you happen to be a chicken or a rabbit.”
Did you know – even the UK Food Standards Agency (FSA) and UK National Health Service (NHS) admit this?
– “However, dietary cholesterol has little effect on blood cholesterol. More important is the amount of saturated fat in your diet”. (National Health Service). (Notice the second sentence? They just couldn’t let the theory go).
– “But the cholesterol we get from our food has much less effect on the level of cholesterol in our blood than the amount of saturated fat we eat”. (Food Standards Agency). (This link may disappear, as the FSA is bowing out of giving nutritional advice).
What the government advice should say is: The body makes cholesterol. The cholesterol you eat has no impact on the level of cholesterol in your blood – not “little”, but “no” – (and we’ve known that all along). And they should also explain how saturated fat can determine blood cholesterol levels and then provide irrefutable evidence that it does. But it must be hard for public health bodies to even go this far. As we saw in a recent thread – the FSA also now accept that there is no limit on the number of eggs we can eat: 
If only Keys had stopped here, but he wanted to find an explanation for heart disease and he was not about to be deterred. For some reason, which I find inexplicable, he then turned to fat (the entire literature on this topic is very vague about “fat” vs. “saturated fat” so his early writings are also very vague on the topic). Here’s a bit of Mensa logic for those who like this kind of thing:
i) Only animal foods contain cholesterol (meat, fish, eggs, dairy). NO non animal foods contain cholesterol.
ii) All animal foods contain fat – saturated and unsaturated. Some may be very low in fat (e.g. white fish), but they all contain some fat.
iii) If there is no link whatsoever between increased consumption of foods containing cholesterol and blood cholesterol levels, there can be no link whatsoever between increased consumption of animal foods and blood cholesterol levels since only animal foods can be increased in consumption to increase consumption of cholesterol!
So, Keys first did the graph that was presented at the Mount Sinai hospital (which is the one shown in the Tom Naughton video and in Dr Robert Lustig’s “Sugar: The Bitter Truth” ) and then went on to do the Seven Countries study – which I have read all twenty volumes of and take apart piece by piece in Chapter Eight of The Obesity Epidemic: What caused it? How can we stop it (on this page).
As Kendrick’s two unbiased seven country studies showed – there is not even an association between saturated fat and heart disease – let alone a causation. However, Keys published his seven countries study and the rest, as they say, is history.
3) The Robert Redford film All the Presidents’ Men that had the memorable quote “follow the money”. This is absolutely at the heart of everything in the diet industry from national dietary organisations to the food, drink and drug industries and individuals in between.
The Ancel Keys work interestingly claimed that saturated fat consumption (A) caused heart disease (C) not directly, but by raising cholesterol (B). Hence A was supposed to cause C through B. For this to even get off the starting blocks, A and C have to be related (plot one against the other and there has to be a clear relationship); A and B have to be related and B and C have to be related. None of these in fact holds. The Kendrick study shows that A and C are not related. There is no logic that A and B could be related – because of the problem of fat and cholesterol being found in the same foods and Kendrick presented many studies that showed B and C were not related. I aim in this article to put the nail in the coffin for any idea that high cholesterol is even associated with high heart disease. We will, in fact, show that the evidence confirms the opposite.
By having cholesterol as this middle-man, this has allowed an entire pharmaceutical industry (and stupid cook books) to come up with ways of lowering cholesterol. The most lucrative of these has clearly been statins – drugs designed to stop the body producing the cholesterol that it is designed to produce. It never hurts to remind people that one statin alone, Lipitor, has been worth $125 billion to Pfizer since 1997. Taubes has a deeply troubling passage in The Diet Delusion where he looked at the committee who approved a lowering of the target cholesterol levels for the USA population. From memory (it’s a big book to find a reference!), a number of people were on the committee and all but one were funded by pharma companies and one didn’t want the target cholesterol level lowered. I wonder which one! (Anyone reading this – if you can find the page number I’d be so grateful – my copy has so many scribbles on I can barely read it).
So, cholesterol will remain the mass murderer for as long as statins are as lucrative as they are or until the public are enlightened and courageous enough to say no to doctors who try to put them on this medication (like my mum was after reading Dr MK!)
A small technicality
On p35 of The Great Cholesterol Con, Kendrick says: “How can eating saturated fat raise LDL levels? It is not merely biologically implausible, it is biologically impossible. Boy does that statement make me a hostage to fortune!”
I arranged to meet a biochemist at a local university to try to get to the bottom of this statement. The biochemist (who has more qualifications than I’ve had dark chocolate) was sadly so brainwashed in the ‘fat is bad’ theory that he just kept saying eating fat raises cholesterol. When I asked him to talk me through the biochemical pathway from fat digestion through to how this impacts cholesterol he said he didn’t know the digestive process well enough – we would need to add a dietician into the conversation. This was alarming enough. I then said – we eat 39 grams of butter per person per week in the UK and about 1.4 kilos of flour – didn’t he think it was more likely that the flour was making us fat and sick. He said it only took a drop of arsenic to kill us. I left shortly afterwards.
Kendrick has to be right (isn’t he always?) LDL (remember this is not cholesterol – it is a low density lipoprotein) is the left over from IDL (intermediate density lipoprotein), which is the left over from VLDL (very low density lipoprotein). VLDL is one of the measures you get in your blood cholesterol test (actually they estimate it – they don’t measure it – they only measure total cholesterol and HDL leaving two other unknowns in an equation with four variables and you thought this was scientific). (They also call VLDL ‘triglyceride’, which is confusing and unhelpful). Cutting a complex story short (it is explained in my book in different passages), carbohydrates can impact VLDL levels (starter for 10: Acetyl-CoA being the start of the process by which the body makes cholesterol and part of the Kreb’s cycle whereby the body turns glucose into ATP), but I really have found no way in which the fat that we eat can do so. Because fat is not water soluble, it is packaged into a lipoprotein in the digestive system. The lipoprotein that fat goes into is the biggest one – the chylomicron – and then it travels off into the body to go and do the essential repair and maintenance jobs that fat does. Does the fat say – hang on Mr chylomicron – we need to go via the liver and see if we can mess up the body’s VLDL production in some way?! Do ask this ‘how’ question (in detail) of someone who thinks that this is possible. I am still open to someone answering this, but I’m not holding my breath.
Fructose, on the other hand, we do know goes straight to the liver to be metabolised. Could that, and other carbs, impact VLDL production? The evidence I have already seen is strong that they do.
The serious bit
The WHO data is split into men and women. I first did the scatter diagrams for average (mean) cholesterol levels and CVD deaths. Then I ran the Pearson correlation coefficient on these numbers. This gives us the term called “r”. “r” tells us if there is some kind of a relationship: an r score of 0 would indicate no relationship; an r score of 1 would indicate a perfect relationship. A negative r score is called an inverse relationship e.g. the price of concert tickets is likely to be inversely related to the number of concert tickets bought – fewer tickets being bought at higher prices.
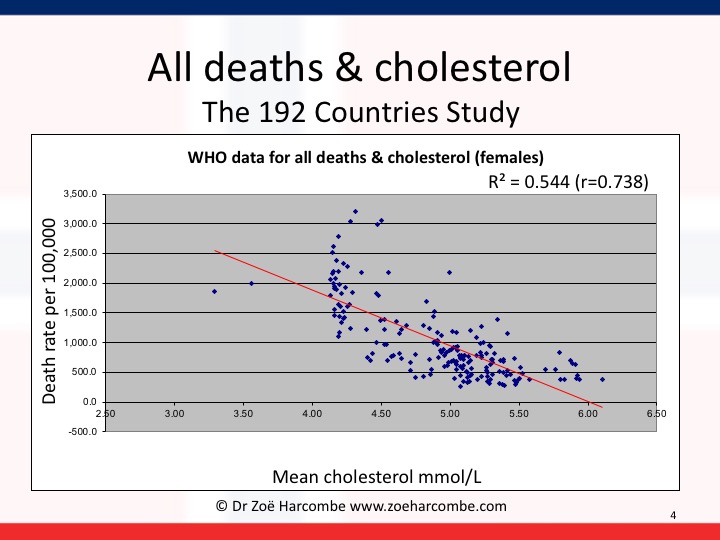
The “r” score for men revealed that there was a small relationship of 0.13 – however this relationship was inverse. The diagram and correlation shows that higher cholesterol levels are associated with lower CVD deaths and lower cholesterol levels are associated with higher CVD deaths. In women, the relationship is stronger – to the point of being meaningful. The r score was 0.52 – but, again, inverse. For women, higher cholesterol levels are quite significantly associated with lower CVD deaths and lower cholesterol levels are quite significantly associated with higher CVD deaths. Please note that I have added r squared on the graphs below (excel can do this for us) and it can confirm that you’ve got your r numbers right and r squared tells us the strength of any relationship we have observed.
All you need to do is to look at the lines going down to the right and wonder how on earth we ever got away with telling people that cholesterol causes heart disease. High cholesterol is associated with lower heart disease and vice versa – for all the data available in the world. High cholesterol is not even associated with high heart disease, let alone does it cause it.


It gets worse. I then kept the cholesterol information and changed the death rates to total deaths – all deaths from any cause – cancer, heart disease, diabetes, strokes – all deaths. You can see the diagrams for men and women again below. This time there is a significant relationship for both men and women: 0.66 for men and 0.74 for women – again inverse. There is a significant association between higher cholesterol levels and lower deaths and lower cholesterol levels and higher deaths for men and an even more significant relationship for women.


This is serious. I’ve shown it to a couple of academics (Professor sort of things) with whom I’ve been having great debates, as I want to see what the view is from people who wholly believe the fat/cholesterol/heart/death hypothesis. (Kendrick talks in his book about what happened when he showed an intelligent colleague his two seven countries studies and the evidence was just dismissed instantly). It is most useful to know what the resistance arguments will be before starting to invite the resistance. The two arguments I got back were:
1) “Ah yes – but this is only an association.”
Ah yes – but a) we changed global dietary advice back in 1977-1983 on the back of an association in Seven (carefully hand picked) Countries that miraculously became a causation even when the association was far from established and b) it is an association that’s the opposite to the one that the world currently holds true and c) that’s what epidemiology is supposed to be about – establish an association and then investigate if there could be any causation or useful learnings. So – go out with a new paradox – that high cholesterol is associated with low deaths and then see what dietary advice emerges.
2) “But that’s total cholesterol – the key thing is the ratio of good to bad cholesterol.”
Oh boy! The chemical formula for cholesterol is C27H46O. There is no good version or bad version. HDL and LDL are not even cholesterol, let alone good cholesterol or bad cholesterol. They are lipoproteins – see above – and they carry cholesterol, triglyceride, phospholipids and protein. Do you think that taxis are people? Or do you think that they are carriers of people (and luggage, and pets and fresh air and other things).
Back to – this is serious. Why are we lowering cholesterol when lower cholesterol is associated with more deaths from heart disease and all causes for men and women?
The doctors’ Hippocratic oath is “First do no harm”.
This also says to me – even though saturated fat has nothing to do with cholesterol, it doesn’t actually matter. Even if it did – cholesterol is only associated with CVD deaths in an inverse way. If fat did raise cholesterol – as public health officials like to claim – it could save lives! Please note I am always really careful with language in this area and never jump from association or relationship to causation. Someone may be in the bath and they may be singing – if we observe this in many cases, we may claim that there is an association. We cannot say that bathing causes singing or that singing causes bathing.
Our global dietary advice was changed in 1977 in the US and 1983 in the UK as a result of a biased study of seven handpicked counties. Had the data been available for the 192 countries we can analyse now, or had Keys even considered all the data that was available to him at the time (for France etc), our conclusion may have been that we need to protect cholesterol levels in the body. We may have realised that the last thing we should be trying to do is lowering cholesterol – unless we’re trying to lower life expectancy for some reason.
Zoë Harcombe



I love Zoe. My BIG question is this: Is the bias against cholesterol based on dead people and the fact that saturated fat solidifies in a corpse? Butter slips between your fingers at body temperature and is such a disco saturated fat. It moves and funks everywhere. I hate to ask the question but are all these studies based on solid saturated fat, cholesterol at room, not body temperature? I wouldn’t put it past the medics. They’re not the best scientists.
Hi Juliet
Thank you!
The history behind the view that cholesterol (and fat/saturated fat) are bad for us was summarised in my PhD thesis.
https://www.zoeharcombe.com/phd-thesis/ Chapter 2 is the one with all the history. If you can’t see this (not sure if you’re a member or if it’s on open view), the references should be on open view. There are many references back to the work of Russian pathologists who found arteries clogged in people who had died suddenly (probably heart attacks, but we didn’t use that term until decades later).
The clogging was made up of a number of things including cholesterol. They hypothesised that cholesterol was the cause. The alternative view is that something damaged the arteries and then repair lipids were sent to the area to fix the damage. Just as fire fighters would be found at the scene of fires, but they didn’t cause the fire.
Best wishes – Zoe
The 2002 stat’s are no longer available, they only go back to 2005 now.
So can you supply the raw data please.
Hi Douglas
I updated the post here https://www.zoeharcombe.com/2021/06/cholesterol-mortality-world-graphs/
This work has mow been published in a peer reviewed journal – handy if you want to cite it Ravnskov et al. The LDL Paradox: Higher LDL-Cholesterol is Associated with Greater Longevity. Annals of Epidemiology & Public Health 2020. https://meddocsonline.org/annals-of-epidemiology-and-public-health/the-LDL-paradox-higher-LDL-cholesterol-is-associated-with-greater-longevity.pd
Best wishes – Zoe
Hi, how did you gather so much knowledge on serotonin, SSRi’s?
Zoe, you have blown my mind! I have been looking for an article that sums up this contentious issue for some time. Your article is clear and easy to ‘digest’. I am a 55 year old healthy male, I have never smoked or consumed alcohol and do regular exercise. I am also a black belt in Karate. For some reason, my five male siblings and I demonstrate high cholesterol readings whenever we have our blood checked. I have long believed that my 8.3 level of ‘bad’ LDL was of no consequence and once again, told my doctor to sit on her recommendation of “life saving statins”.
Thank you for a great piece of science based writing.
Pingback: Why you should ignore the government's nutritional guidelines Episode 83 - Culinary Libertarian
Pingback: Cholestérol et maladies cardiaques - il y a une relation, mais ce n'est pas ce que vous pensez
Pingback: Cholestérol et maladies cardiaques - il y a une relation, mais ce n'est pas ce que vous pensez
Pingback: Vegan Plan - The Complete Guide to Saturated Fat
Zoe, thanks for this article. I note the graphs stop plotting cholesterol around 6. Did the data show cholesterol levels out further to 8,9,10? Can the same trends conclusions be seen?
Hi Chris
The cholesterol numbers on the WHO data were means for each country, so no mean exceeded those shown just beyond 6. I’ve gone back to the original data for interest and – in men – the highest countries were Columbia, Serbia Montenegro, Luxembourg and Uruguay – at 6 or slightly above. For women – Norway was the only one with a mean over 6 although Luxembourg and Uruguay were just under 6.
Best wishes – Zoe
Thanks Zoe, Your a lifesaver. My Doc advised me to take statins, But after further thinking i realised that my doctor hadn’t even run blood tests for my original concern. He appeared to have only done the bare minimun tests to allow him to suggest my colesterol was high. When i ask him about my original concerns which were all available through blood tests, They hadn’t been performed. I’m so greatful to have come across your site it stemmed a lot of worry and put be back on track.
I did have my doubts about medical advice anyway as i realise money controls everything. You might be interested in the corbettreport.com. He is not a professional or specialised like yourself, but he does interview people that are and all his work has references and and real documentation that you can follow and research yourself. He covers all kinds of conspiracies but one that may be of interest to yourself is “Rockefeller Medicine” Link is…https://www.youtube.com/watch?time_continue=2603&v=X6J_7PvWoMw. It’s not junk and contains varied and detailed information from various sorces.
I’m not affilliated (or even a member for that matter) to the site but it does mention the California university that i seem to remember in some of your research.
Hi David
You may like this post too!
https://www.zoeharcombe.com/2015/03/worried-about-cholesterol-andor-statins/
Many thanks for your tip back – I’ll check that out.
Best wishes – Zoe
Hi Zoe, Just an update on my issue. When my doc sent me an email suggesting i take statins, he also sent a link to an NHS site to explain statins. When i looked over that site it suggested that if i had an underactive thyroid then statins would not be given to me as the cholesterol issue will be addresed with the medication for underactive thyroid. This test was never done so i insisted that it was done with another blood test. With a mainly negative attitude with this idea i was tested and found to have an underactive thyroid.
This is just to vindicate your approach Zoe, that is, it doesn’t hurt to do your own research as you can always express it to your doctor and compare his/her explanation to your concerns. Had i not have discovered your site i would now be regularly taking statins leaving the real issue (which sounds just as dangerous when you read about it) undiagnosed.
Again, a big thanks Zoe, and all the best to you and your team. Truly brilliant.
Hi Dave
Well done to you for working out the puzzle and getting such a good result. And thank you for your kind words.
Best wishes – Zoe
Pingback: My Cholesterol Levels Part 2: Examining My Need For Statins - Gluten Free Homestead
I’m concerned about my cholesterol levels as they’ve been going up for the past few years. I’m 62, 5’4 and weigh 136 lbs. my total cholesterol was 319 this time and my doctor has prescribed of course, Lipitor. I do not want to take a statin but am nervous that my cholesterol is rising. I have changed my diet according to my GP, low carb, sugar etc. And eating more of a Mediterranean diet so why is my cholesterol going up? Should I go back to eating more fat etc and just not worry about it at all. Stress has played quite a large part in my life this past few years too due to ill health of my mother, but my doctor doesn’t seem to have taken this into account either. She just keeps saying you don’t want a stroke do you?. Well of course not!
Hi Lynn
I wrote this post to put in one place info on cholesterol/statins – I hope it is of interest: https://www.zoeharcombe.com/2015/03/worried-about-cholesterol-andor-statins/
Stress will have made a difference (and I’m sorry to hear why). Sun exposure would make a difference – maybe you’ve been too busy caring to sunbathe? You could be eating less stuff that contains plant sterols – plant sterols artificially lower cholesterol but the impact on actual events is not good (https://thescipub.com/abstract/10.3844/ojbsci.2014.167.169).
There are many doctors who would be pleased that your cholesterol is rising as you age – low cholesterol for people over 70 is particularly associated with poor outcomes (https://bmjopen.bmj.com/content/6/6/e010401)
My money would be on sun and stress – but that’s just my opinion.
Good luck with your continued exploration to learn in this area.
Best wishes – Zoe
Thank you – this and the other articles relating to cholesterol lay out the data and hypotheses very well. I am trying to get a broad understanding of where the ‘cholesterol myth’ comes from for some academic work in this area (I’m in my first year Nutrition undergrad.) This has all helped a great deal as a jumping off point. I have just one question: lots of the literature I have read suggests that our body makes 40% of the total cholesterol we need; it is a figure that has come up repeatedly. If dietary cholesterol does not in any way effect serum cholesterol then where does the other 60% come from, (or rather, where does this figure originate?)
Thanks and Regards!
Hi Victoria
You’ll know that there are essential nutrients, which means something that we must consume in nutrition. Cholesterol is so essential (in the normal meaning of the word) that the body doesn’t risk leaving it to chance that we would need to consume cholesterol. Left to its own devices (i.e. without statins and the likes) the body will make all that we need. If we consume cholesterol, we do the body a favour because it then needs to make less.
I’ve not seen the 60% figure. With a quick search, there’s 75% here: https://www.healthline.com/health/where-is-cholesterol-found#sources
I’m sure there will be other numbers. The bottom line is that the body will make 100% of what it needs if allowed to do so and if it needs to.
Best wishes – Zoe
How can we say no to the Doctor that wants to put you on satins? Once you do it they dismiss you as a patient and god knows we do need doctors from time to time.
Hi Ana
This may help with more ammunition https://www.zoeharcombe.com/2015/03/worried-about-cholesterol-andor-statins/
If you’re UK based, there is a big thing at the moment on patient informed choice and the doctor is supposed to inform you to help you to make your own choice. I’ve heard of some cases when people enlightened about cholesterol listened politely and then said no thanks to statins and there was no reaction. My best friend has just been to the GP for the first time in years and was having a cholesterol test before she realised and then just smiled politely at the chat that followed! (cholesterol of 4 would be better than 5 kind of insanity!)
I have also heard of ‘devious compliance’ – some people take the prescription and then just don’t go to the pharmacy to get the drugs. Doc is happy, patient is happy – only the drug co is not happy!
These are anecdotes not advice! You’re the patient – you decide :-)
Best wishes – Zoe
I am in US. There is a big cholesterol harassment going on here. I am resisting it, hoping that soon this “high cholesterol” theory will change. But the scary part is that in the midtime they are getting to our children with this “high cholesterol” harassment.
I am not a researcher and not a doctor, but I do have analytical mind and my thinking is that something else is causing this “bad” cholesterol to stick to blood vessels in some people and they yet have to find what is this, what is this disorder. And I guess those people have to keep their “bad” cholesterol as low as possible, till other cure is found. But brashing everybody under the “high cholesterol” theory and medicating everybody is wrong.
It is very sad that we cannot trust our doctors these days and have to become our own doctors, that can be dangerous.
In US people are overmedicated. They are popping pills like candy.
Hi Ana – you’ve worked it out! That post (https://www.zoeharcombe.com/2015/03/worried-about-cholesterol-andor-statins/) leads you off to other thinkers in this field. I highly recommend Dr Malcolm Kendrick – he was the one who first opened my eyes on cholesterol! He has a new book out soon too – can’t wait!
Best wishes – Zoe
Well your graphs just clarify even further that CVD is pretty much non-existent below 4 mmol, which is basically a physiologically normal level.
https://www.ncbi.nlm.nih.gov/pubmed/15172426
http://circ.ahajournals.org/content/circulationaha/108/22/2757.full.pdf
The “normal” is considered by the general public, not by evolution.
I had a heart attack when my level was 4.4 mmol. It’s been consistently below 3 mmol for the last 10 years with no new heart disease or progression of disease in an artery that was slightly blocked before. No other health concerns either, for that matter.
Hi there, thanks for the great article. I have a question I’m hoping you
might be able to answer. I was wondering, What is the difference between panic attacks and anxiety attacks?
I definitely get one of the other but I’m unsure which…
I would appreciate any insight you can provide.
Am trying to locate the datasets referred to [clipped below]. Failed to do so :-( Suspect WHO website restructured since original article post. Can anyone help with a few URLs? Thanks.
Greg
“You go to the WHO statistics area of their web site and then pick data for cholesterol from risk factors (how judgemental to start with!) and then look under: Global burden of disease (mortality); All causes; Non communicable diseases and then G Cardiovascular disease (shortened to CVD). CVD deaths include ischemic heart disease and cerebrovascular disease – that means fatal heart attacks and fatal strokes to us. You find the most recent year where you can get both sets of data to compare like with like. This turns out to be 2002. You download their very user friendly spreadsheet data (CSV) – cut and paste it into an excel file and then try to remember how the heck to do scatter diagrams in excel!”
Hi Greg
Funnily enough this is on my TODO list to revise.
I’ve got a word pad ready with these as possible new links (you’re right – they very annoyingly had a site restructure)
Mean cholesterol: http://www.who.int/gho/ncd/risk_factors/cholesterol_prevalence/en/
NCDs: http://www.who.int/gho/ncd/mortality_morbidity/ncd_total/en/
I wouldn’t be surprised if my comparison is no longer possible. The European heart data for sat fat and CHD stopped being updated – can’t think why!
https://www.zoeharcombe.com/2015/03/saturated-fat-chd-in-europe/
Best wishes – Zoe
p.s. I’ve got the original spreadsheets if they help with anything you’re researching?
Hello Zoe,
I’m convinced in almost all what you’ve said about Cholesterol theory.
Too much interested in your opinions and looking forward to know how to read our HDL, LDL, Triglycerides levels.
I did a test recently and found the below values: HDL 42, LDL 145, TC 227 and TG 196.
I have few questions for you:
1. according to your findings, lowering total HDL+LDL values is not important? will not have any positive impact on our health?
2. if 2 persons have the same total TC, but person 1 has more HDL than person 2, should not we consider that person 1 is in a better health than person 2?
3. I did not see in your conclusions anything about Triglycerides? should they follow the same Cholesterol theory or really we should lower as much as possible TG levels?
Regards,
Wissam
Hi Wissam
This is my main post on cholesterol/statins https://www.zoeharcombe.com/2015/03/worried-about-cholesterol-andor-statins/
It starts with my view that we are better off not knowing any of the things you have shared!
On your (very good!) questions:
1) I do not think lowering cholesterol (total, HDL, LDL etc) is of any value. Certain methods may do more harm (http://thescipub.com/abstract/10.3844/ojbsci.2014.167.169) There may be a benefit of statins because of their anti-inflammatory properties (still likely not worth the side effects) but the cholesterol lowering is a by-product (and not a good one).
2) This is what surprised me about the inverse relationship in this post (which I did not expect to find). Knowing the role of cholesterol, I would expect the body to make more cholesterol if someone needed more. You would expect the person who needed more to be less healthy in some way (ill, stressed, had an operation, got damage to repair etc) Therefore I would expect high cholesterol to be a marker of poorer health but, for all the countries in the world, this is not the case!
3) Trigs are worth worrying about because they are a marker of carb intake. Again – they should not be lowered artificially (if there were a pill to lower trigs for example) – the person should eat fewer carbs and then trigs will lower naturally. The health benefit is in eating fewer carbs – the lower trigs is just a marker.
Best wishes – Zoe
My question is, do we know what we can do to lower our risk of heart disease if saturated fat and cholesterol have nothing to do with it? Beyond the obvious not smoking, where does maintaining a healthy weight, consistent exercise, and eating fruits and vegetables stand? Do those things actually help? I guess it’s impossible to know since it is so hard to do studied without third variable issues.
Hi Kimberly
This brilliant series explores possible pathways…
https://drmalcolmkendrick.org/2016/01/18/what-causes-heart-disease/
He’s now up to part XXXIII https://drmalcolmkendrick.org/2017/07/29/what-causes-heart-disease-part-xxxiii/
So plenty of reading!
Best wishes – Zoe
France wouldn’t prove Keys wrong. In France just like elsewhere those with higher cholesterol levels do have an increased risk of CHD (Ducimetiere, 1980, Lancet). It was also found they underreport heart disease (Burr, 1995). An interesting piece has been written about this in dialogues cvm (dcvm49)
“CONCLUSION Returning to the question raised in the introduction of this review, we can now say that CHD rates are not so low in France, animal fat intake not so high, and the diet-heart concept not so unique that the existence of a “French paradox” may be sustained any longer, except as cultural fantasy or a marketing ploy”
France also has the famous Lyon Trial where butter was replaced with a canola oil based margarine among other things and the experimental group experienced significantly fewer cardiac events.
It isn’t a single country that is a paradox, Keys cherry picked 7 countries for his revalations but over 20 countries data was available. If all available stat’s are compared his theory no longer has a clear association with fat or cholesterol. The association that stands out is sugar. I think that is a clear correlation, but that does not prove causation and where are the trials? Keys had no real correlation and the trials have not proven his hypothesis, most don’t prove anything due to poor set up and, or lack of significant difference in results.
Under and over reporting is always an issue. Many, many people just die with no clear reason and if no autopsy is performed doctors often put the latest fashionable reason why people die.
No autopsy in an unknown cause of death, what you say? If old age is a factor this is common and if you are very old what does it matter. You got to be very old and have to die of something. We should exclude the very old from the stat’s. My father in law at 96 died after having coved, but he had recovered from the virus, but died a couple of weeks later. He had also fallen over and fractured his hip and was operated on post coved. So what should we report and how does it relate to me at 69 or anyone young
Hi Douglas
You may enjoy this https://www.zoeharcombe.com/2017/02/keys-six-countries-graph/
Six countries vs the seven countries study – different, but one led to the other.
Best wishes – Zoe
Interesting, but I would take it with a pinch of salt as Yudkin using the full available stat’s pointed out that the correlation with fat did not actually exist and that there was a more likely correlation with sugar and cvd. Keys confronted with this attacked Yudkin so Keys had all the stat’s at that point and still stood by the lesser stat’s.
Both of course need proof as “correlation does not prove causation”
Could I please ask your opinion about Lp(a)? I have been on Lipitor (generic) for many years. My brother had a massive stroke at 55 years of age last year. We do seem to have FH. He was never overweight, exercised plenty, did not take statins because they made him hurt. His cholesterol at the time of the stroke was well over 300. I will be 60 in August and when I told my doc about the stroke he tested my Lp(a). It was 158 and should be less than 30. From reading about it, it’s nearly impossible to bring this number down. He says to take a supplement called heart plus and CoQ 10. So, would stopping the statins hurt in this case? It’s just so confusing and now I feel kind of like a walking time bomb. Thanks for any advice you can give.
Hi Gabrielle
For Lp(a) – I would put that term into the search box on this site (https://drmalcolmkendrick.org/) Dr Malcolm Kendrick first alerted me to the fact that Lp(a) likely is an important measure. He can tell you more – I haven’t studied it personally.
On FH – this may be of interest: https://www.zoeharcombe.com/2016/11/familial-hypercholesterolemia-fh/
You may like this quote in the article: “The combined findings from these two Simon Broome Register Group papers show that, if you genuinely have FH and you are aged 60 or over you should be pleased to know that you have a lower risk of cancer and no greater risk of heart disease.”
On how statins work (and why anyone on statins should also be on CoQ10) – this may be of interest: https://www.zoeharcombe.com/2013/10/how-statin-drugs-really-lower-cholesterol-and-kill-you-one-cell-at-a-time/
This is my main post on everything statins and cholesterol: https://www.zoeharcombe.com/2015/03/worried-about-cholesterol-andor-statins/
One of the links in that post takes you to this article: http://bmjopen.bmj.com/content/5/9/e007118.full
People on statins may gain 3-4 days in 5 years. Worth the side effects?!
Not in my view – but it’s your call!
Hope this is of interest.
Best wishes – Zoe
Pingback: The Complete Guide to Saturated Fat
Hi Zoe,
I’m very interested in the data you have, but in the end, it’s just another tiny piece of the massive jigsaw that is human biology. There are _SO_ many variables that it is impossible (with our current technological limitations) to standardise any study on dietary factors. There is so much still understood, but at least with work like yours the traditional views prevalent from about the 70s are starting to unravel.
Some of your replies are also interesting and some people still don’t realise that one swallow does not make a summer.
Pingback: The crosswalk paradox, cholesterol myths and risk management – Environmental Resource Systems Analysis Group
I am having trouble accessing this data, there appears to be no details for risk factors or cholesterol on the page you link to. Any help appreciated.
Hi Mark
It appears WHO have updated their site.
This is where the WHO link used to go to (https://web.archive.org/web/20150403135652/https://apps.who.int/infobase/Comparisons.aspx) – snap shot, so the data won’t be accessible. I’ve emailed health info at WHO to see if the data are still available somewhere else on the site. I’ll update the link if it is.
Meanwhile cholesterol as a ‘risk factor’ is here http://apps.who.int/gho/data/node.main.A867?lang=en
and the CVD mortality data are here http://apps.who.int/gho/data/node.main.A865CARDIOVASCULAR?lang=en
Just not as user friendly as the previous link.
Best wishes – Zoe
Low cholesterol causes death by cancer and other diseases or other diseases cause low cholesterol, which comes first the chicken or the egg ?. This study suggests an answer
http://circ.ahajournals.org/content/92/9/2396
In this piece of research below the extact opposite is reported, cholesterol increase go’s hand in hand with CVD deaths. What or who are we to believe
http://jn.nutrition.org/content/128/2/444S.full
Firstly this an article not a piece of research. It just reports on the opinions of the people they mention. What you need to do is investigate the research used as proof by the mentioned people to reach their conclusions.
There are number of books that cover this including one of Zoe’s.
Question everything. If there is no real evidence either way, then the body must have its cholesterol level for a reason.
I am enjoying your articles. However, I have a small issue with one logical argument you made along the lines of; study proved dietary cholesterol doesn’t cause CVD, all dietary cholesterol comes from animals which also have animal fat, therefore study also proved animal fat doesn’t cause CVD. My issue is that the ratio of cholesterol to fat is not constant in all animal food sources, so your conclusion is not necessarily true. For example, shrimp has a much higher ratio than beef, so if the study was conducted with high percentage of calories from dietary shrimp, the conclusion wouldn’t necessarily apply to a diet high in beef. Having said that, I think your conclusion has been thoroughly proven from other studies! Best, John
One other reply you get from Cholesterol theory supporters is that lower cholesterol readings meaning greater death rates overall is skewed by reverse causation. In other words if you are ill and about to die your cholesterol levels will take a hammering and thus hey presto low cholesterol si associated with mortality.
Any views on this idea ?
Hi Mark
I struggle to see how this could be argued at a whole population level (which is what these charts are about). However I struggle to see the whole cholesterol theory!
Remember the CHEST study? Where they measured the LDL of people arriving at hospital having a heart attack?
The conclusion of the study was:
“Young adults experiencing acute MIs typically have acceptable cholesterol levels (i.e.< 130 mg/dL) or optimal values (i.e. < 100 mg/dL)”. (Kwame O. et al, Chest 2001;120;1953-1958) The initial CHEST study was quite small, but the goal was considered to be important to understand. Hence the net was cast more widely to gather far more data on cholesterol levels of people admitted to hospital with heart attacks. Data was subsequently gathered from 231,986 hospital admissions, across 541 hospitals. The lipid levels were documented in 136,905 cases (allowing for VLDL, LDL, HDL etc levels to be known). The average LDL levels were 104.9mg/dl. In UK speak this is 2.6mmol/l. (American Heart Journal 2009;157:111-7.e2) 70% of the people admitted to hospital having a heart attack had an LDL level below the average (the “mean” for the statisticians among us). Half of the people arriving at hospital with a heart attack had an LDL level below 100mg/dl (2.5mmol/l in UK language). Hence, people with so called ‘optimal/ideal’ LDL levels were at the same risk of MI (heart attack) as people with higher LDL. You would think that, with such a magnitude of data and overwhelming evidence, the conclusion would be – one’s LDL appears to have bugger all to do with one’s chance of having a heart attack, Except, perhaps, low cholesterol may not be as favourable as high. The conclusion was, however, that these findings may provide support for even lower LDL goals! That's why you can't try to apply logic with the cholesterol hypothesis creators! Best wishes - Zoe
I was there (ie, a first-year grad student in genetics, forced to take a graduate course in biochemistry, in 1966-67) when the first publication relating blood cholesterol vs heart attacks was published. The lecturer lampooned that study, firstly on the grounds that cholesterol is vital (as is amply defended above) and secondly because the authors fitted a single straight line to their data, thereby giving an X-axis intercept — a “safe” level of blood cholesterol, when in fact a straight line (no relevance) would have been equally defensible. *This* is where the fixation that “total cholesterol” mattered entered the mainstream of dialogue, whereas we now know (citations needed) that only cholesterol that has interacted with oxygen (something we also cannot live without) actually matters. We (humans, all higher forms) cannot break down those fairly common side reactions. But others can, and use them for energy, otherwise we would be stuck in a sea of oxydized cholesterol soup. Some of those “others” have been identified. I’ve pushed my personal connections as far as I can, given my conscience. Goole me to find the links.
Hi Adelaide – thanks so much for sharing this – a fellow Cambridge Uni person! I like the X-axis intercept bit – the graphs that derive from the WHO data in this post imply that there is a cholesterol level at which no deaths would occur, which is clearly absurd! However, I did not expect to find an inverse relationship when I plotted them. I didn’t know what I’d find – which is what research is supposed to be!
Best wishes – Zoe
Hi Zoe
I came across you article while searching for cholesterol levels and mortality. I remeber seeing a graph whereby a level of 6.5 carried the lowest mortality rates with a steep rise on the lower side and a gradual rise on the upper levels, I still haven’t managed to find it.
This was in response to the article published in the Lancet this week stating that using statins prevent 1000 heart attacks/strokes in 10,000 (high risk group) and 500 in 10,000, in low risk. Also they state that in the control group there were almost as many reports of side effects than the statin group. What are your observations in this report?, it seems to be based on the hypothesis that reducing cholesterol, reduces risk of these events. I cannot understand how they can put together all the studies carried out and come up with a report that shows the benefits of statins are far greater by a huge amount than even the most pro statin study.
I have been looking for the study over 5 yrs that came to the conclusion that there was a 30% improvement using statins, but looking at the detail the figures were something like 329 deaths in the statin group, compared to 334 in the control group in a study of 10.000 people, and the results (RR) used by GPs’ as the Gold standard in the argument for prescribing statins. Do you know where I can find this ?
My doctor has prescribed statins, but they lie unopened in the draw. No matter how hard I look, I cannot find a good case to take a drug that affects the livers production of cholesterol, which is needed throughout the body for cell health and repair, all arguments seem to fly in the face of common sense.
Respectfully yours Dave Williams
Hi Dave
Was it not the graphs on the post that you’ve commented on? Scroll down… https://www.zoeharcombe.com/2010/11/cholesterol-heart-disease-there-is-a-relationship-but-its-not-what-you-think/
I’ve dissected the latest study here (https://www.zoeharcombe.com/2016/09/the-lancet-statin-study/) but this one if for subscribers, not on open view – I sadly need to earn a living!
I don’t know the precise 329 vs 334 study that you mention – but that’s a fairly typical use of relative risk, as I frequently point out with studies.
You may also find this useful – on open view https://www.zoeharcombe.com/2015/03/worried-about-cholesterol-andor-statins/
Best wishes – Zoe
Hi Zoe, noted your graph, but the one I saw ranged from zero to about 20, and just had a curve.
Interesting article today in the NYT
The sugar industry paid scientists in the 1960s to play down the link between sugar and heart disease and promote saturated fat as the culprit instead, newly released historical documents show.
The internal sugar industry documents, recently discovered by a researcher at the University of California, San Francisco, and published Monday in JAMA Internal Medicine, suggest that five decades of research into the role of nutrition and heart disease, including many of today’s dietary recommendations, may have been largely shaped by the sugar industry.
“They were able to derail the discussion about sugar for decades,” said Stanton Glantz, a professor of medicine at U.C.S.F. and an author of the JAMA Internal Medicine paper.
The documents show that a trade group called the Sugar Research Foundation, known today as the Sugar Association, paid three Harvard scientists the equivalent of about $50,000 in today’s dollars to publish a 1967 review of research on sugar, fat and heart disease. The studies used in the review were handpicked by the sugar group, and the article, which was published in the prestigious New England Journal of Medicine, minimized the link between sugar and heart health and cast aspersions on the role of saturated fat.
Even though the influence-peddling revealed in the documents dates back nearly 50 years, more recent reports show that the food industry has continued to influence nutrition science.
Last year, an article in The New York Times revealed that Coca-Cola, the world’s largest producer of sugary beverages, had provided millions of dollars in funding to researchers who sought to play down the link between sugary drinks and obesity. In June, The Associated Press reported that candy makers were funding studies that claimed that children who eat candy tend to weigh less than those who do not.
The Harvard scientists and the sugar executives with whom they collaborated are no longer alive. One of the scientists who was paid by the sugar industry was D. Mark Hegsted, who went on to become the head of nutrition at the United States Department of Agriculture, where in 1977 he helped draft the forerunner to the federal government’s dietary guidelines. Another was Dr. Fredrick J. Stare, the chairman of Harvard’s nutrition department.
Hi Dr Harcombe
Have just re-read your article again, again – even more fascinating than the first time. Dr Kendrick (as you probably know, but a reader may be interested) has just completed a series of 20 articles on why we get heart disease. Also absolutely fascinating. Cholesterol is no a cause!.
robert
Hi Robert – we’re been following Malcolm’s series avidly – brilliant isn’t it!
Best wishes – Zoe
He says stress is the cause. Therefore if we believe all this stuff about cholesterol our stress will fall. We take statins and our stress will fall as we will believe all will be OK. Our cholesterol will further fall owing to statins which will further reduce stress.
Therefore this blog is doing a huge disservice.