
Cholesterol & heart disease – there is a relationship, but it’s not what you think
This post is dedicated to Anne who asked me a great question about cholesterol. It made me do what I had been meaning to do ever since I read Dr Malcolm Kendrick’s The Great Cholesterol Con…
Dr MK ran some analysis on World Health Organisation (WHO) data. The WHO has extensive data from almost 200 countries on more health measures than you could imagine – definitely worth a look one rainy, wintry afternoon. This is where Dr MK presented the world with two different Seven Country Studies – (for those of you who aren’t familiar with the history, it was the Ancel Keys’ Seven Countries Study that started all the fat heart hypothesis stuff). Dr MK took the seven countries with the lowest saturated fat intake and then the seven countries with the highest saturated fat intake. You may need to read this twice – but he found: “Every single one of the seven countries with the lowest saturated fat consumption has significantly higher rates of heart disease than every single one of the countries with the highest saturated fat consumption.”
The next chapter in The Great Cholesterol Con goes on to look at cholesterol and heart disease (and overall death rates) and quotes many great studies where it is shown that lower cholesterol is associated with higher mortality. However, it did leave me thinking – having run the data on saturated fat and heart disease, let’s just run all the data on the cholesterol and heart disease and get to the bottom of this hypothesis from all parts of the allegations.
It actually didn’t take that long – less than a couple of hours one Saturday afternoon. You go to the WHO statistics area of their web site and then pick data for cholesterol from risk factors (how judgemental to start with!) and then look under: Global burden of disease (mortality); All causes; Non communicable diseases and then G Cardiovascular disease (shortened to CVD). CVD deaths include ischemic heart disease and cerebrovascular disease – that means fatal heart attacks and fatal strokes to us. You find the most recent year where you can get both sets of data to compare like with like. This turns out to be 2002. You download their very user friendly spreadsheet data (CSV) – cut and paste it into an excel file and then try to remember how the heck to do scatter diagrams in excel!
Before telling you the results, we need to go back for a quick reminder on what we know about cholesterol and then hopefully this can serve as a factsheet for all the cholesterol questions we continually get.
The role of cholesterol
It is virtually impossible to explain how vital cholesterol is to the human body. If you had no cholesterol in your body you would be dead. Every single cell of your body is covered by a membrane (think of a membrane as the ‘skin’ or protective barrier around each cell). This membrane is made largely of cholesterol, fat and protein. Membranes are porous structures, not solid walls, letting nutrients and hormones in while keeping waste and toxins out. If cholesterol were removed from cell membranes they would literally explode from their internal water pressure. Human beings quite simply die without cholesterol.
Cholesterol is vital for hormone production – the sex hormones and therefore the entire human reproductive system are totally dependent on cholesterol. Hence, not only would humans die without cholesterol, the human race would die out.
Cholesterol is vital for digestion. The human body uses cholesterol to synthesise bile acids. Without cholesterol-rich, bile salts, the human body could not absorb essential fatty acids or the fat soluble vitamins (A, D, E and K) and serious, even life threatening, deficiencies could develop. (It is interesting, therefore, that nature puts cholesterol in virtually every food that contains fat – providing a digestion mechanism in tandem).
Cholesterol is vital for the brain, central nervous system and memory functions (hence how the side effects of statins include memory loss, mental confusion and people generally just not feeling themselves). Even though the brain is only 2% of the body’s weight, it contains approximately 25% of the body’s cholesterol. The vital connections between nerve endings in the brain, which help to conduct the electrical impulses that make movement, sensation, thinking, learning, and remembering possible, are largely made up of cholesterol.
Cholesterol is critical for bones and for all the roles performed by vitamin D. Vitamin D is best known for its role in calcium and phosphorus metabolism, and thus bone health, but we are continually learning more about potential additional health benefits of vitamin D from mental health to immune health. Vitamin D can be ingested (and is, interestingly again, found in foods high in cholesterol) and it can be made from skin cholesterol. Modern ‘health’ advice to avoid the sun, take cholesterol-lowering drugs, eat a low cholesterol diet (whatever the heck that is supposed to be) – combined with there not even being a recommended dietary allowance for vitamin D – is undoubtedly contributing to avoidable modern illness.
One of the key reasons that we need to spend approximately one third of our lives sleeping is to give the body time to produce cholesterol, repair cells and perform other essential maintenance.
This gives you the headlines of the vital functions that cholesterol performs, but hang on to that bottom line – it is utterly vital and we die instantly without it.
You may be familiar with the term essential fatty acids or essential amino acids (proteins break down into amino acids). The term ‘essential’ used like this in nutrition means that it is essential that we consume it in our diet because the body can’t make it. The body makes cholesterol. That says to me that cholesterol is even more vital than essential fatty acids or essential amino acids – even though these too are life critical – and therefore the design of the human body is such that it was not left to chance that we needed to get cholesterol from food. Of the 500 or so roles that the liver has – one is to produce cholesterol. It is too vital to be left to chance.
What went wrong?
So, how did something so life vital become more vilified than a mass murderer? I think it comes down to three things (and I don’t take credit for this view – it is there to be worked out by anyone who traces back the history and Kendrick, Uffe Ravnskov and all the thincs.org guys have led the way):
1) Rabbits;
2) Ancel Keys;
3) Money!
1) In 1913, a Russian chap called Nikolai Anitschkow decided to feed rabbits purified cholesterol and he managed to get their blood cholesterol levels in excess of 1,000 mg/dl (nearly 26 mmol/L! Most UK people have levels of 5-7 mmol/L). He then noticed the formation of “vascular lesions closely resembling those of human atherosclerosis” forming in the arteries of the rabbits. The obvious flaw in the experiment should have been that rabbits are strict herbivores. They do not eat animal products, which is the only source of cholesterol. Hence rabbits are in no way designed to digest cholesterol or animal fat and no one should be surprised if cholesterol or animal fat ended up stuck in any part of the poor rabbit. The only surprise is that no one thought to ask Anitschkow why he was feeding cholesterol and animal fat to herbivores. Interestingly, far less well known is that a parallel test was done on rats and dogs (omnivores) and feeding cholesterol to these species failed to produce lesions.
2) Ancel Keys. Remember the Minnesota experiment that I so often refer to? A brilliant and unbiased piece of research, which has given the world one of the best insights into low calorie dieting ever done – it was pure genius. This study made Ancel Keys the man of the moment and I guess he wanted to follow it with something equally impactful. There is an anecdote in The Great Cholesterol Con and on p113 of The Obesity Epidemic where Henry Blackburn, one of Keys’ closest colleagues, tries to explain what may have fuelled Keys drive to find a connection between diet and heart disease.
What is little known is that Keys originally tried to establish a link between cholesterol in food and cholesterol in the blood (our cholesterol levels when we have a blood test) because he thought (probably because of poor Bugs Bunny) that cholesterol in the blood causes heart disease.
Keys did multiples of studies, changing the diets of his human ‘guinea pigs’, and he presented his conclusions in The Journal of Nutrition, November 1955: “It is concluded that in adult men the serum cholesterol level is essentially independent of the cholesterol intake over the whole range of natural human diets. It is probable that infants, children and women are similar.” i.e. I only tested adult men and there is no relationship between cholesterol eaten and cholesterol in the blood and it is probable that there will similarly be no relationship for women or children.
In 1997 Keys put this even more assertively: “There’s no connection whatsoever between cholesterol in food and cholesterol in blood. And we’ve known that all along. Cholesterol in the diet doesn’t matter at all unless you happen to be a chicken or a rabbit.”
Did you know – even the UK Food Standards Agency (FSA) and UK National Health Service (NHS) admit this?
– “However, dietary cholesterol has little effect on blood cholesterol. More important is the amount of saturated fat in your diet”. (National Health Service). (Notice the second sentence? They just couldn’t let the theory go).
– “But the cholesterol we get from our food has much less effect on the level of cholesterol in our blood than the amount of saturated fat we eat”. (Food Standards Agency). (This link may disappear, as the FSA is bowing out of giving nutritional advice).
What the government advice should say is: The body makes cholesterol. The cholesterol you eat has no impact on the level of cholesterol in your blood – not “little”, but “no” – (and we’ve known that all along). And they should also explain how saturated fat can determine blood cholesterol levels and then provide irrefutable evidence that it does. But it must be hard for public health bodies to even go this far. As we saw in a recent thread – the FSA also now accept that there is no limit on the number of eggs we can eat: 
If only Keys had stopped here, but he wanted to find an explanation for heart disease and he was not about to be deterred. For some reason, which I find inexplicable, he then turned to fat (the entire literature on this topic is very vague about “fat” vs. “saturated fat” so his early writings are also very vague on the topic). Here’s a bit of Mensa logic for those who like this kind of thing:
i) Only animal foods contain cholesterol (meat, fish, eggs, dairy). NO non animal foods contain cholesterol.
ii) All animal foods contain fat – saturated and unsaturated. Some may be very low in fat (e.g. white fish), but they all contain some fat.
iii) If there is no link whatsoever between increased consumption of foods containing cholesterol and blood cholesterol levels, there can be no link whatsoever between increased consumption of animal foods and blood cholesterol levels since only animal foods can be increased in consumption to increase consumption of cholesterol!
So, Keys first did the graph that was presented at the Mount Sinai hospital (which is the one shown in the Tom Naughton video and in Dr Robert Lustig’s “Sugar: The Bitter Truth” ) and then went on to do the Seven Countries study – which I have read all twenty volumes of and take apart piece by piece in Chapter Eight of The Obesity Epidemic: What caused it? How can we stop it (on this page).
As Kendrick’s two unbiased seven country studies showed – there is not even an association between saturated fat and heart disease – let alone a causation. However, Keys published his seven countries study and the rest, as they say, is history.
3) The Robert Redford film All the Presidents’ Men that had the memorable quote “follow the money”. This is absolutely at the heart of everything in the diet industry from national dietary organisations to the food, drink and drug industries and individuals in between.
The Ancel Keys work interestingly claimed that saturated fat consumption (A) caused heart disease (C) not directly, but by raising cholesterol (B). Hence A was supposed to cause C through B. For this to even get off the starting blocks, A and C have to be related (plot one against the other and there has to be a clear relationship); A and B have to be related and B and C have to be related. None of these in fact holds. The Kendrick study shows that A and C are not related. There is no logic that A and B could be related – because of the problem of fat and cholesterol being found in the same foods and Kendrick presented many studies that showed B and C were not related. I aim in this article to put the nail in the coffin for any idea that high cholesterol is even associated with high heart disease. We will, in fact, show that the evidence confirms the opposite.
By having cholesterol as this middle-man, this has allowed an entire pharmaceutical industry (and stupid cook books) to come up with ways of lowering cholesterol. The most lucrative of these has clearly been statins – drugs designed to stop the body producing the cholesterol that it is designed to produce. It never hurts to remind people that one statin alone, Lipitor, has been worth $125 billion to Pfizer since 1997. Taubes has a deeply troubling passage in The Diet Delusion where he looked at the committee who approved a lowering of the target cholesterol levels for the USA population. From memory (it’s a big book to find a reference!), a number of people were on the committee and all but one were funded by pharma companies and one didn’t want the target cholesterol level lowered. I wonder which one! (Anyone reading this – if you can find the page number I’d be so grateful – my copy has so many scribbles on I can barely read it).
So, cholesterol will remain the mass murderer for as long as statins are as lucrative as they are or until the public are enlightened and courageous enough to say no to doctors who try to put them on this medication (like my mum was after reading Dr MK!)
A small technicality
On p35 of The Great Cholesterol Con, Kendrick says: “How can eating saturated fat raise LDL levels? It is not merely biologically implausible, it is biologically impossible. Boy does that statement make me a hostage to fortune!”
I arranged to meet a biochemist at a local university to try to get to the bottom of this statement. The biochemist (who has more qualifications than I’ve had dark chocolate) was sadly so brainwashed in the ‘fat is bad’ theory that he just kept saying eating fat raises cholesterol. When I asked him to talk me through the biochemical pathway from fat digestion through to how this impacts cholesterol he said he didn’t know the digestive process well enough – we would need to add a dietician into the conversation. This was alarming enough. I then said – we eat 39 grams of butter per person per week in the UK and about 1.4 kilos of flour – didn’t he think it was more likely that the flour was making us fat and sick. He said it only took a drop of arsenic to kill us. I left shortly afterwards.
Kendrick has to be right (isn’t he always?) LDL (remember this is not cholesterol – it is a low density lipoprotein) is the left over from IDL (intermediate density lipoprotein), which is the left over from VLDL (very low density lipoprotein). VLDL is one of the measures you get in your blood cholesterol test (actually they estimate it – they don’t measure it – they only measure total cholesterol and HDL leaving two other unknowns in an equation with four variables and you thought this was scientific). (They also call VLDL ‘triglyceride’, which is confusing and unhelpful). Cutting a complex story short (it is explained in my book in different passages), carbohydrates can impact VLDL levels (starter for 10: Acetyl-CoA being the start of the process by which the body makes cholesterol and part of the Kreb’s cycle whereby the body turns glucose into ATP), but I really have found no way in which the fat that we eat can do so. Because fat is not water soluble, it is packaged into a lipoprotein in the digestive system. The lipoprotein that fat goes into is the biggest one – the chylomicron – and then it travels off into the body to go and do the essential repair and maintenance jobs that fat does. Does the fat say – hang on Mr chylomicron – we need to go via the liver and see if we can mess up the body’s VLDL production in some way?! Do ask this ‘how’ question (in detail) of someone who thinks that this is possible. I am still open to someone answering this, but I’m not holding my breath.
Fructose, on the other hand, we do know goes straight to the liver to be metabolised. Could that, and other carbs, impact VLDL production? The evidence I have already seen is strong that they do.
The serious bit
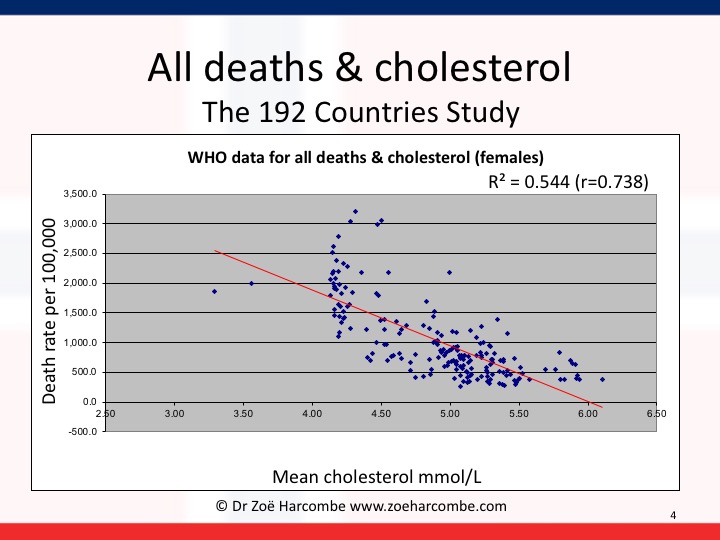
The WHO data is split into men and women. I first did the scatter diagrams for average (mean) cholesterol levels and CVD deaths. Then I ran the Pearson correlation coefficient on these numbers. This gives us the term called “r”. “r” tells us if there is some kind of a relationship: an r score of 0 would indicate no relationship; an r score of 1 would indicate a perfect relationship. A negative r score is called an inverse relationship e.g. the price of concert tickets is likely to be inversely related to the number of concert tickets bought – fewer tickets being bought at higher prices.
The “r” score for men revealed that there was a small relationship of 0.13 – however this relationship was inverse. The diagram and correlation shows that higher cholesterol levels are associated with lower CVD deaths and lower cholesterol levels are associated with higher CVD deaths. In women, the relationship is stronger – to the point of being meaningful. The r score was 0.52 – but, again, inverse. For women, higher cholesterol levels are quite significantly associated with lower CVD deaths and lower cholesterol levels are quite significantly associated with higher CVD deaths. Please note that I have added r squared on the graphs below (excel can do this for us) and it can confirm that you’ve got your r numbers right and r squared tells us the strength of any relationship we have observed.
All you need to do is to look at the lines going down to the right and wonder how on earth we ever got away with telling people that cholesterol causes heart disease. High cholesterol is associated with lower heart disease and vice versa – for all the data available in the world. High cholesterol is not even associated with high heart disease, let alone does it cause it.


It gets worse. I then kept the cholesterol information and changed the death rates to total deaths – all deaths from any cause – cancer, heart disease, diabetes, strokes – all deaths. You can see the diagrams for men and women again below. This time there is a significant relationship for both men and women: 0.66 for men and 0.74 for women – again inverse. There is a significant association between higher cholesterol levels and lower deaths and lower cholesterol levels and higher deaths for men and an even more significant relationship for women.


This is serious. I’ve shown it to a couple of academics (Professor sort of things) with whom I’ve been having great debates, as I want to see what the view is from people who wholly believe the fat/cholesterol/heart/death hypothesis. (Kendrick talks in his book about what happened when he showed an intelligent colleague his two seven countries studies and the evidence was just dismissed instantly). It is most useful to know what the resistance arguments will be before starting to invite the resistance. The two arguments I got back were:
1) “Ah yes – but this is only an association.”
Ah yes – but a) we changed global dietary advice back in 1977-1983 on the back of an association in Seven (carefully hand picked) Countries that miraculously became a causation even when the association was far from established and b) it is an association that’s the opposite to the one that the world currently holds true and c) that’s what epidemiology is supposed to be about – establish an association and then investigate if there could be any causation or useful learnings. So – go out with a new paradox – that high cholesterol is associated with low deaths and then see what dietary advice emerges.
2) “But that’s total cholesterol – the key thing is the ratio of good to bad cholesterol.”
Oh boy! The chemical formula for cholesterol is C27H46O. There is no good version or bad version. HDL and LDL are not even cholesterol, let alone good cholesterol or bad cholesterol. They are lipoproteins – see above – and they carry cholesterol, triglyceride, phospholipids and protein. Do you think that taxis are people? Or do you think that they are carriers of people (and luggage, and pets and fresh air and other things).
Back to – this is serious. Why are we lowering cholesterol when lower cholesterol is associated with more deaths from heart disease and all causes for men and women?
The doctors’ Hippocratic oath is “First do no harm”.
This also says to me – even though saturated fat has nothing to do with cholesterol, it doesn’t actually matter. Even if it did – cholesterol is only associated with CVD deaths in an inverse way. If fat did raise cholesterol – as public health officials like to claim – it could save lives! Please note I am always really careful with language in this area and never jump from association or relationship to causation. Someone may be in the bath and they may be singing – if we observe this in many cases, we may claim that there is an association. We cannot say that bathing causes singing or that singing causes bathing.
Our global dietary advice was changed in 1977 in the US and 1983 in the UK as a result of a biased study of seven handpicked counties. Had the data been available for the 192 countries we can analyse now, or had Keys even considered all the data that was available to him at the time (for France etc), our conclusion may have been that we need to protect cholesterol levels in the body. We may have realised that the last thing we should be trying to do is lowering cholesterol – unless we’re trying to lower life expectancy for some reason.
Zoë Harcombe


Hi Zoe,
I am 51 and my Father died suddenly of a heart attack at the same age. This provides me with some anxiety and a little obsession. He was a very heavy smoker, didn’t exercise that much, and a little over weight. Dont know how stressed he was but possible.
I have high cholesterol but dont want statins and so tend to avoide the GP! I want to have an idea of how worried I should be about the hereditary connection between me and my father? Should I be demanding having any medical tests? I have also smoked but gave up 5 years ago. I would also like to consider what I can do to best prevent having a heart attack. One main idea seems to be stress reduction, others relate to potassium and certain levels of vitamins.
Any links advice etc would be much appreciated.
Many thanks,
John
Hi John
I can’t give advice but I can share info/views and I’m very sorry to hear how prematurely your dad died.
This is my signpost article on cholesterol and statins https://www.zoeharcombe.com/2015/03/worried-about-cholesterol-andor-statins/
(Do check out the “how statins really work” and check whether your cholesterol is genuinely high – double figures consistently – or just high relative to moved goal posts… and anything else of interest)
As an outside observation – the worst thing your dad did was to smoke. The best thing you did was to give up. If there is a hereditary/genetic heart condition that both of you have (and dad could have had something from his lineage, which you haven’t inherited), I’m sorry to say there’s probably not much you can do (except make the best of the genes you have by not smoking/eating well/managing stress/doing natural activity – walking etc/getting a dog etc…)
Lowering cholesterol won’t help anything IMHO!
Best wishes – Zoe
Hi Zoë,
Thank you for the video I just watched on YouTube, regarding responses to sling, when people think you are batty, to say we can lose weight on a LCHF diet. My usual response is, ‘Well it’s me who is losing the weight, I am happy to be batty!’
Now I can say ‘Show me the evidence!’ Especially to a certain Nutritionist Phd, on another forum, who doesn’t like being taken to task by ‘unqualified, ignoramuses (Or is that ignoramusii? :) )
Thanks again. and take care.
John Walker
Oh – do name! ;-)
Pingback: Scared back to Fitness – HeartHomeandStuff
Your topic in this article is clear. I’m wondering though if you offer any research/commentary on what causes artery disease? I’m a skeptic, so I’m looking for your I -depth review and opinion on what actually causes plaque to accumulate in arteries (chemically/biologically) vs the reasons given by all the governing agencies and for-profit sources. Thanks
Hi Melonie
This is the definitive blog series answering that question – and showing how complex it is. The blog series is up to part XVIII – https://drmalcolmkendrick.org/2016/07/12/what-causes-heart-disease-past-xviii/
Start from the beginning!
This is a very short hand version: https://www.zoeharcombe.com/the-knowledge/fat-does-not-clog-up-our-arteries/
Best wishes – Zoe
Pingback: Open Letter Response to CMS on MACRA & MIPS | Taking Back Medicine
Zoe,
I love your work. I only wish I understood it better! I am no scientist so may be missing something… I get the NO STATINS fact. I tell that to everyone I know. Are you saying, though 1) “high” cholesterol is good – depending upon the person’s “normal levels of cholesterol (which many don’t know their normal as they haven not been tracking for life so who can say they are high?) OR are you saying 2) lower “high” cholesterol by increasing fibre foods and GETTING RID OF chemicals/ processed sugars i.e white bread foods. So, in other words, don’t worry about high cholesterol stop eating garbage and you’ll be fine.
Hi Sophia
Many thanks for your lovely comment. My basic message is – I wish people didn’t even know what their cholesterol was and then they wouldn’t worry about it!
This post may help: https://www.zoeharcombe.com/2015/03/worried-about-cholesterol-andor-statins/
To answer your questions specifically – I would deffo agree with the final sentence: “don’t worry about cholesterol stop eating garbage” I can’t say that you’ll be fine ‘cos you may have bad genes, or be elderly or be a smoker – or all sorts of other things, but don’t eat rubbish and don’t worry about cholesterol is a good summary.
1) The “high chol is good” is an interesting question. I was surprised by these graphs to be honest. I actually think that cholesterol may be a health MARKER – just not a health MAKER. I think that genuinely high cholesterol (not 7-8 which is pretty normal for pre-statin levels) is the body trying to tell us something. Cholesterol should rise when we are ill/injured – to repair us. Hence high cholesterol can be a MARKER that something else is going on. It doesn’t cause anything – it’s trying to tell us something.
2) Which is why I don’t think we should try to lower cholesterol with meds or fake foods. If cholesterol falls because we eat better and therefore have better health – so be it. But we really should not try to lower it as an activity in itself. Eat well, move, don’t smoke, sleep, have loved ones etc- and cholesterol will be what it will be.
Hope this helps!
Best wishes – Zoe
Pingback: Sugar is the new fat – WIBN
Thanks for sharing this nice article it have some great useful blog….
Thanks for this great article. I am a type 2 diabetic who switched to a low carb diet about 2 1/2 years ago. I now no longer need insulin and have the best blood sugar readings since my diagnosis 12 years ago. My cholesterol was below 4 as I was taking a statin. After switching to a low carb diet it went up a little to around 4.5. I then decided to stop taking the statin and it shot up to 7.4. Should I be worried? I have my annual check up soon and I suspect my doctor will advise me to start the statin again.
Hi Paul
Well done for these incredible blood glucose health results – that alone should extend your life and healthy years…
On the cholesterol/statins, this may help https://www.zoeharcombe.com/2015/03/worried-about-cholesterol-andor-statins/
Personally I would not worry for one second about any cholesterol reading – the world would be a much better place if we had never decided to measure it. This post has links to all the key things I’ve written about this topic (and recommendations for other viewing/reading). Check out the link to the BMJ paper on the 19% inaccuracy of the whole test – your doc probably won’t know that. 7.4 is bang normal (but normal has been moved so that you can be a medication opportunity). Even if it is 7.4 – that would be like me being the average height 5’4″ as opposed to 5’2″ or 5’6″ – the normal distribution has people at the norm and people either side – that’s why it’s normal!
If you live in the UK you’re a bit stuffed before the test because a great way to lower cholesterol is to sunbathe. This makes vit D (which is what’s healthy) – the fact that your cholesterol will drop is an inevitable consequence of making vit D but it keeps dull doctors happy!
This is why I avoid docs!
Best wishes – Zoe
Hi Zoe.
Saturated fat does in fact raise LDL cholesterol.
The mechanism is simple and has been known for a long time.
Chylomicron remnants, ie what remains to be processed by the liver after the chylomicron has cycled through the lymph and plasma is actually taken up by hepatic LDL receptors. Thus there is competition for these LDL receptors from returning LDL AND these chylomicron remnants. This reduces the catabolic rate of LDL but does not affect the production rate. Therefore the LDL pool rises until the rates are again balanced.
I can supply the references if interested.
Thanks.
Tim.
Hi Tim
Yes please can you share references
Many thanks – zoe
I’m an active 34 year old Male and my LDL cholesterol has been creeping up over the last few years to 213 and my HDL is 45 and Triglycerides 130, BP is 120/88, I got gym 6 days a week alternate running and weights, am generally active outside of gym, don’t’ smoke and eat healthy 90% of time with very little junk food or snacks, Dr wants me to start treatments and not sure what to do?
Hello,
Congratulations on your post, was very informative. I have recently made blood test and my total cholesterol level was 265, HDL cholesterol – 65 and LDL cholesterol – 171. My doctor prescribed me atorvastatin but I am a 22 years old male. My mother also as high cholesterol in the family so my doctors thinks the best solution is medication. I am a little resilient on statin medication, so how can i change my diet in order to lower my cholesterol or is it in my best interest to lower it?
Best regards,
Hi Rúben
This will tell you what I think about cholesterol!
https://www.zoeharcombe.com/2015/03/worried-about-cholesterol-andor-statins/
Best wishes – Zoe
I have just got back from attending the first day of the HeartUK conference which is drug company sponsored Cholesterol festival. I asked questions related to some of the topics on here eg why are we measuring basic cholesterol numbers when even in the cholesterol field there are better indicators, indeed one researcher in the afternoon showed that Lp(a) was second only to smoking as an indicator of future heart disease. I was literally laughed at by doctors in the audience and after posing my third question of the morning one doctor then put his hand up and said that after hearing what I had to say he would now have to consider that the earth is flat. When I engaged with him afterwards to have a sensible debate he would not talk to me and simply walked away. It may well be that we wont get a real sea change until this generation of doctors die off and the next come through.
Pingback: Sugar is the new fat | nutrilicious
Re Nathan Pritikin – his diet may have lowered his cholesterol but he had cancer (leukemia) – ? related to low cholesterol ? In any event, he committed suicide so lowering his cholesterol didn’t exactly do him much good in the long run
Somehow this cholesterol “bad” for health has been misleading us for decade by those pharmaceutical co through so called healthy advisory. Same goes the decade old food pyramid. Which I have throw those grains 5 serving intake to the least 1 serving making it 5 servings meats, milk and eggs intake.
Hi Zoe, I loved your article.
Ive recently been to the Gp post a blood test in which my LDL was 6.8 (Australian ratios) and she wanted me to go onto a Statin.
I said Nooooooo.
Hence I’ve since gone down the track of a Naturopath and looked at the link between “Leaky gut and increased cholesterol levels”
Im on a path to decrease the Inflammation level in my body and so far Im feeling much much better.
My Gp wants a repeat cholesterol level done in 3 months so Im determined to flaw her.
High cholesterol is in my family.
My Dad had it and so did my Mum.
Both my parents had a Sweet Tooth and have passed that on to their 7 children.
In know that four of the seven have high Cholesterol.
My Mum died recently of a stroke at the age of 88…. but the interesting thing is that she was on a high dose of Lipitor for years since she had a CABG when she was 73.
She was living independently but gradually declining cognitively…. She then had a sudden period of confusion and so called Psychosis. This was followed by very uncharacteristic aggression and paranoia, so the Gp put her onto an antipsychotic drug which a side effect of increased her chance of Stroke. She was labelled with Aggressive Dementia…. and ended up in a Dementia Unit… So within 3 months of all this appearing… she had gone from a fully functioning 88yr old love to an unpredictable individual…. BUT she remembered people and everything that happened the day before! She just didn’t fit the picture of DEMENTIA….
I believe she suffered from the Side effects of Lipitor… no one investigated that.
They were all to concerned with her Behaviour and labelling her.
So in the end she had the stroke that was warned to us that she might have if she went on the Antipsychotic meds. (It was the drug with the less side effects that was recommended).
I found your article so interesting because it makes sense doesn’t it… as a society we have growing obesity, we consume fast food and eat sugar even in foods that look healthy i.e: low fat yoghurt, we have inactivity and we have increasing Dementia!!!!
The evidence is glaringly obvious!
Thank you Vicki!
You may like this one too: https://www.zoeharcombe.com/2013/10/how-statin-drugs-really-lower-cholesterol-and-kill-you-one-cell-at-a-time/
And here’s a summary of pretty much all the cholesterol stuff on my site: https://www.zoeharcombe.com/2015/03/worried-about-cholesterol-andor-statins/
You may like to check out this guy too – http://healthinsightuk.org/2014/08/20/keeping-my-dad-alert-an-unconventional-and-successful-approach-to-dementia/
Done some really interesting stuff about fats and dementia
Best wishes – Zoe
You’re dead wrong and it’s kind of scary.
Several points:
1. An r value of 0.52 is not indicative of a “significant association” – inverse or otherwise.
2. Weight loss is associated with lower cholesterol, and many millions of people around the world die of starvation.
3. Many millions of people around the world also die of diseases like TB, cancers, HIV/AIDS, and diarrhea, and serious disease processes like these cause low cholesterol.
In statistics there are things called “confounders”. If you bothered to look up the definition of “r value” maybe you could bother with confounding factors too.
AC, you might want to look up critical sample size for r. When you do, you will find that an r-value of 0.52 is statistically significant with a sample size of 12. As you can see, the sample size is much greater.
If you were using the term “significant” in a more colloquial sense, then I still believe you’re incorrect. For a dependent variable as complex as mortality, it is absurd to think that any single independent variable would account for the majority of variance in mortality. So, accounting for 25% of the variance is actually quite large (i.e. significant).
Confounders are clearly an issue. However, the advantage of Ms. Harcombe’s simplistic approach is that it includes data from 2/3 world countries and well as industrialized countries, so the analysis gives a robust look at the relation between cholesterol and mortality globally. Similar findings were just published by Petursson et al. from data in Norwegians.
Weight loss is not equivalent to starvation. So unless you can provide a reason that the lower cholesterol data comes largely from people who are starving, then your proposition is merely conjecture.
Perhaps you could supply us with a peer-reviewed study that has controlled for all the confounders you’ve listed and has included data from all the countries, or at least global regions included in Ms. Harcombe’s analysis.
The criticism you offer does little to move the discussion forward if you don’t offer a better option.
The relation between cholesterol and mortality is clearly not settled, but throwing out the word “confounder” does little to dismiss the general relation shown.
Perhaps a little more circumspection in your comments
I am confused about what makes cholesterol levels go up. If “there’s no connection whatsoever between cholesterol in food and cholesterol in blood” then why do the French or Italians and others have higher cholesterol than say the Chinese. This is not a question about cholesterol being a culprit, but why such varying levels.
Maybe this is a stupid question but I can’t see an answer.
thanks
Gwen
Hi Gwen
Interesting question. The examples you’ve picked unfortunately don’t make the case: Cholesterol levels in China are 5.39 for men/5.22 for women; France is 5.46 for men/5.36 for women; Italy is 5.22 for men 5.14 for women, but I know what you’re asking. (The blog shares how to download the data and then you can check each country).
Lowest for men is Cameroon (2.99). Highest for men is Colombia (6.22 mmol/L). I found an almost perfect correlation between latitude and cholesterol levels (and CHD), which held for the 7 countries study but wouldn’t hold for these 2 countries – both v close to the equator. What else is going on? Genetics and stress would be my top 2 suggestions.
Best wishes – Zoe
Chris Masterjohn reckons that around 20% of people are hyper responders to dietary cholesterol and I think he might be right. One week I ate eggs for breakfast every day and had two liver evening meals and my LDL went from 3.0mmol to 4.0mmol
Hi Mark
Check out the work of Dave Feldman in hyper response – he’s mastered it!
Best wishes – Zoe
http://cholesterolcode.com/
Question please: Recently our Family Doctor a D. O. tested my cholesterol and said it was 177. He said; dietary changes are needed, I told him how I eat on a daily basis he then said, if you indeed eat that way every day then your genetics tells me you’re a candidate for a pill. My question is, how can I eat, live, and/or exist and be able to get their numbers down to stay away from those drugs?
Hi Timothy
If 177 mg/dl (US) (4.5 mmol/L (UK)) was your total cholesterol reading, then you are well below normal. This recent post may help with all the nonsense going on: https://www.zoeharcombe.com/2015/03/worried-about-cholesterol-andor-statins/
It will hopefully help you realise that your body is making cholesterol – let it do what it was designed to do and understand that the winners in the ‘getting the numbers down game’ are the pharma giants
Best wishes – Zoe
I have just read your fine article will a great sense of relief. I’m now 73 and quite active: gardening, walking (including moubntain walking) and the kind of fishing that involves walking a lot. After being badgered by my doctor for a couple of years about my high cholesterol – c. 5.5 total – I finally agreed to start taking statins as the dic saiod that I had a one in four chance of a coronary event otherwise. The real clincher however was a summary study by people at Johns Hopkins who collated and analysed all published studies of statins over the last 25 years. The interesting statistic was that their analysis suggested (95% confidence limit), that taking statins appeared to reduce the risk of both dementia and colo-rectal cancer by as much as 65%. Given that both are complete disasters, I thought I’d go with the statins. In all I tried three sorts, all of which made me utterly wretched in that I felt both ill and depressed; the second one coincided with a fall in my plate count to around 120 along with bone deep fatigue etc. Within a week of giving up on these I felt much better and blood tests showed tht my plate count was continuing to rise. I am now takiong something called Crestor which is the least bad, probably because I take it every other day rather than as prescribed. My father ate everything, saw a doctor maybe four times in his 89 years and grew his own food. I grow some of my own food and cook on a daily basis, everything from fillet steak to roast lamb, and various Chinese and Italian inspired collations. Until I started taking statins I doubt I’d had a days illness in my life. In October I went for a third blood test to check the progress of my plate count. To cut a long story short, the nurse complained that my veins werte small, was not able to obtain a sample and on the second try in my left arm subjected me to excruciating pain. I began to develop all manner of pains in that arm and was unable to straighten it without pain; In view of this I refused to take another blood test. A few days ago I went to a Chinese herbalist that I know; she carried out an acupuncture routine and now all previous symptoms have gone; she told me I had suffered nerve damage. The following day I saw my doctor and he was most offhand when I explained that I had refused the blood test in January because of previous events. Interestingly, my sister told me that her partner, a supoer-fit builder had an identical experience when giving blood and was unable to worl for almost a month. I intend to (a) stop taking statins and (b) cut down on products containing flour, though I make my own bread (one multiseed, one white with rye) and eat a slice of each at breakfast; I’m hoping this is not regarded as excessive. My problem is that I’m worried that my doctor is going to become difficult over me not taking his ‘advice’.
Hi Mike
Almost all statins are not advised for over 70’s – even the patient leaflets acknowledge this. Your doc needs to read more patient leaflets. Crestor is not as explicit as some I’ve seen (https://www.medicines.org.uk/emc/PIL.11972.latest.pdf). This one says “Warnings and precautions…Talk to your doctor or pharmacist before taking CRESTOR…If you are over 70…” but adds that this is so that the doc can choose the right dose. In my opinion the right dose for anyone over 70 is no statins! You’ve already experienced the side effects. How much more nerve damage, muscle ache (known statin side effects) do you need to experience before your doc treats you as a person and not as a prescribed intervention?
Google “low cholesterol and mortality in the elderly”(http://www.thelancet.com/journals/lancet/article/PIIS0140-6736%2801%2905553-2/fulltext?). Particularly in older people – low cholesterol is associated with high mortality – you’ll find plenty more evidence to support this Lancet article. I’d be considering a law suit against the doctor – not worrying about him becoming difficult! Seriously – some docs are so blinkered in their view of cholesterol/statins, they are not treating people any more.
Best wishes – Zoe
p.s. Given the impairment of mind and memory, it is far more likely that statins are implicated in dementia (http://www.scientificamerican.com/article/its-not-dementia-its-your-heart-medication/)
Hi Zoe,
The US dietary guidelines were changed, but it seems like they are still saying saturated fat is bad for you. Should we be following the new changes? Is there still misinformation in this article?
Excerpt:
However, this does not mean that people can start eating foods high in saturated fat, which are a major source of “bad” LDL cholesterol , warned Dr. Robert Eckel, chair of atherosclerosis for the University of Colorado Anschutz Medical Campus and a spokesman for the AHA.
“Saturated fat is still bad for your blood cholesterol,” as are trans fats, he said.
http://www.webmd.com/cholesterol-management/news/20150210/us-advisers-rethink-cholesterol-risk-from-foods-report?page=3
Hi Shawn – there’s still loads of ignorance about what sat fat even is – it’s one of three natural healthy fats. The only one you need to avoid is the man made one – trans fats.
Robert needs to read this! https://www.zoeharcombe.com/2013/09/why-the-australian-heart-foundation-wont-have-evidence-against-saturated-fat/
Best wishes – Zoe
Pingback: Heart disease risk on my low-carb, high fat diet - Rogue Health and Fitness
Pingback: Una curiosidad sobre el colesterol | No vuelvo a engordar
I’ve looked at the graphs and have a problem seeing the significance of the data. My immediate reaction is to mistrust the usage of the data. I make the following points.
1. You use death rates rather than age at death. People at age 80 with a high death rate must be preferable to people at age 8 having a high death rate. So using death rate as opposed to age at death gives us no real feel for the effect of cholesterol on deaths within the population.
2. There is no information on the distribution of cholesterol within the population
3. So why are there dots all over the place surely there can’t be more than one level of death rate for a single level of cholesterol- more than one reading would average out – so why aren’t we seeing the average for each level of cholesterol?
4. Because each level of cholesterol is not set at an even increment from the next, then the usefulness of the scattered points would appear to be questionable. Clearly if the spacing of the statistical “buckets” varies then this would seriously affect the relationship. Put simply if the are two low level points close together – this would equate to one higher point with wider spacing. If one applied that to the graphs it would appear to show an almost normal distribution – which really just tells us that the death rate relates to cholesterol in the same way that the cholesterol level is spread through the population – ie Normally.
However having made my points can I thank you for an excellent discussion
Hi David
Hopefully the final point (for which I think you) is the relevant one – the discussion that can follow from this. The only data I had to work with was that from the WHO (sourced in the post) – mean cholesterol for each of 192 countries and overall death rates for each country. The only split was men/women heart deaths and all-cause mortality.
The most interesting thing for me was that it was not the trend that we are told (and to be honest, what I expected to find before I started the plots). Despite not buying the whole cholesterol con, I did not expect the trends to be in the opposite direction – worth discussion!
Best wishes – Zoe
A friend of mine advocates your way of eating. As the daughter of a dad who died at 52 of a heart attack I’m terrified that if I don’t lower my cholesterol which currently lies at 7.4 I’m going to be in serious trouble in the not too distant future. I’m obese and I would class myself as a food addict although perhaps greedy would be more accurate. I know that I can happily loose a stone or two on a diet and all of a sudden all I can think of is the food, usually a Chinese takeaway. Will this way of living really save me?
Hi Leanne
I’m really sorry to hear you lost your dad at such a young age. I wouldn’t worry about your cholesterol (which is quite normal – they just keep making normal high https://www.zoeharcombe.com/2014/06/diabetes-cholesterol-bp-normal-is-no-longer-normal/) I would worry about what you eat – that will do the harm.
My first book, Why do you overeat? When all you want is to be slim is all about food addiction and physical reasons for it – an emotional ones. I don’t think that people are generally greedy. I do think that processed food (Especially sugar/flour) is addictive and I explain why I think this in the books. I’ll drop you an email to get your address to send you one. I’m not going to make any grand claims that this can save you, but I can say that it can show you a way out of where you are now and the decision is then yours.
Bye for now – Zoe
Thank you Zoe for your reply and the kind offer of your book. I’ve already ordered a copy along with Stop Counting Calories and Start Losing Weight. The evidence of success is certainly there where my friend is concerned and I am hoping that I’ll be able to follow suit. Not only does she look fantastic, she feels really healthy too.
Thanks again,
Leanne.
Pleasure! :-)
Back in the late 1970’s I began to study the science of Dr. Carey Reams and his approach called the Reams Biological Theory of Ionization. There are a good number of websites that discuss it in detail. At that time I started to used distilled water systematically as Dr. Reams taught. His findings were that arteries get plaqued up from salt damage and that distilled water washes out the excess salt, thereby allowing the arteries to be normal and even release the built up plaque back into the bloodstream. In 2009 the VA hospital (I have never been hospitalized) did ultrasounds on my carotids and heart arteries. They found zero cholesterol in them. But I have high cholesterol and a family history of heart disease. Keep up the good work and hope this info helps your readers.
Dear Zoe,
I really appreciate the information you have on your site. I am a doctor and have long suspected that sugar and refined processed food is the enemy more than (if at all) animal fat in terms of cardiovascular disease. If this is the case, there should be a correlation between the increased amounts of sugar consumption by country and cardiovascular or all cause mortality. Can you repeat your WHO data correlation for the same countries and publish these graphs? Although you are (I suspect) right about fat not being the culprit or cholesterol being good or bad, I suspect statins have a strong role to play independent of their cholesterol lowering ability. This may be just a marker of their effect rather than the beneficial intervention they cause. This is likely to be due to lowering inflammatory markers in people who’s diet is dominated by pro-inflammatory processed sugar laden foods. Let’s not throw the baby out with the bath water as there is plenty of evidence for statins lowering mortality.
Hi Jonathan – I’ll stick the sugar one on the todo list – I’ll get told off by my PhD supervisor if I work on other things! ;-)
I agree with you on the likely mechanism by which statins have their known and small ‘benefit’ among men of a certain age who have already had a heart attack – the anti-inflammatory action (and this is known by the statin companies – hence the diversion into arthritis applications). The cholesterol lowering is a serious side effect. The data should be presented to people as – if you’re not in this high risk group don’t even think about statins and if you are in this high risk group and you take a statin for 5-6 years, 98.2/100 of you will receive no benefit (http://drmalcolmkendrick.org/2014/12/01/what-is-t/) and the likelihood of these side effects (memory loss, fatigue, muscle aches & wasting, dementia, impaired cognitive ability, loss of sexual performance/interest) is 1 in X… Then people could make an informed choice. For as long as 28% of Americans are taking a drug that will, in virtually all cases, do more harm than good, I will continue to be an outspoken critic! And – as you imply – wouldn’t it be great if the inflammatory factors (sugar, smoking, stress…) were managed instead.
Best wishes – Zoe
http://rawfoodsos.com/2011/12/22/the-truth-about-ancel-keys-weve-all-got-it-wrong/
I found this blog that seems like you would be interested in reading. It provides a bit more detail about Ancel studies, but it disagrees with a few of the points you made about animal protein and heart disease.
Zoe,
What is your comment on the China study which is one of the largest long term studies that provided a correlation between what people eat and their cancer rates, as well as heart disease.
Hi Shawn – this is the definitive response to the China Study – by the brilliant Denise Minger. http://rawfoodsos.com/2010/07/07/the-china-study-fact-or-fallac/
Enjoy!
Zoe
Zoe,
As a person who was recently diagnosed with high cholesterol, I find it interesting to see that there is no real link between cholesterol levels and heart disease. I’d love to talk to you more so I can inform my family and friends who all believe this to be true. I look forward to reading more of your informative articles. It is nice to see someone who is willing to listen to both sides of an argument and debate. Too many people focus solely on their side and their side only and are too stubborn to look at facts.
A great article ,I am reading Malcolm Kendicks book,it hasn’t all sunk in yet but I will reread it until it does.
I am 67 [ i was going to lie [I still think and act like a kid]
I had my first heart attack in 2004,got a couple of stents for that one.
Then in 2009 had another one ,got a few more stents,and all was fine
I put these attacks down to heavy smoking ,bad diet,and maybe a few beers.I stopped smoking 18 months ago.
I have been on statins for a few years,10mg I could handle,but after another cholesterol test the dose was increased,20mg was the next step,six months ago it was changed to 40mg,
That was disaster for me ,the side affects were horrendous,[I didnt know it was the stain that caused it]I am on a number of other drugs as well.I decided to stop taking the statin and started to feel pretty good after a while.
The thing is,I went to the A&E with typical hart attack pain three months ago,I was kept in over night,and informed it might have been a blood clot on my lung ,no further action.
I had a appointment with my nurse for the flue jab,three weeks ago,I had developed shingles, it never rains but it pours for me.I then had another blood test and was told to come back in a few weeks.
t
The chest pain returned,and my gtn spray helped a bit.this went on for a week or so,
until it woke me up one night and reluctantly phoned for a ambulance.
The paramedics came done a few tests,said I was in the middle of yet another heart attack,
blue lights and all that ,I was in the theater 30 minuets later,getting a blood clot out of my heart,just in time they said,I am now recovering.
Sorry its a bit long winded,but while in hospital I thought maybe not taking the statin has caused this.A fellow patient lent me a copy of dr Kendricks book,what a eye opener it turned out to be.And I firmly believe everything he wrote,
But if I had been a fatality ,and they found out I was not taking my statin,that would be a point for the bad guys.
On leaving hospital I was given 80mg of statin to take for a indefinite period ,they went in the bin.
In conclusion I had to see the cardiac rehabilitation nurse last week,she was more than a bit put out about not taking statin,and a bit of a debate took place,I had done quite a bit of research by then,so held up quite well against the use of satin.
The best part was when she brought up my cholesterol levels on her computer,from three weeks ago,a cholesterol level of 4,she couldn’t explain it,my body done it on its own. She recons in ten years the whole country will take statins,I replied with or no one will be taking them,
The pharmaceutical company’s have created this myth that has gotten so big its hard to disbelieve ,respect to the people that are trying to get this myth out into the open.
Hi, I have cholestrol of 8.4 – am a 54 year old female. Should I be worried. Dont want to take statins. I also have high blood pressure, take meds for these, but would like to come off them.
Hi Biddy – I can’t advise anyone. I just share what I find. This may also be of interest – https://www.zoeharcombe.com/2014/06/diabetes-cholesterol-bp-normal-is-no-longer-normal/
Your BP may not be high – it may just be redefined as high. The post may be of interest for the same having happened with cholesterol (8.4 being normal by definition because it’s in the normal range). Plus – the cholesterol test is so inaccurate – you could go back next week and it be 20% different! (http://www.bmj.com/content/298/6689/1659)
The best things that you can do are: eat real food (not processed junk); don’t smoke; walk and be naturally active (cleaning, gardening, carrying etc). Dropping carbs will have an impact on BP naturally.
Best wishes – Zoe
Pingback: En defensa de la comida tradicional: Sr@s Salud Pública, grasa saturada no es igual a trans | COMIDAS QUE CURAN
Dear Zoe,
Thank you very much for this fascinating and very reassuring article. I had a blood test the other day and was alarmed to receive a letter asking me to see my GP at my earliest convenience. When I went back I saw a different GP who said that my own doctor had been concerned by the high level of cholesterol in my blood. I was staggered by this as I eat an extremely healthy diet, so asked for an explanation. The second GP looked up a chart very similar to the ones above and said that in fact, my ‘high cholesterol level’ (6.2 HDL) meant that actually I couldn’t be healthier and my risk of CVD was so low that I didn’t even figure on the chart!
I was very relieved but at the same time extremely annoyed to have been needlessly alarmed by my own GP, who probably shares many of the misconceptions about cholesterol and gets very well-paid for the privilege!
Keep up the good work.
Regards
Catherine Gale
Hi interesting reading. My wife carol who is diabetic has been taking simfastatin for some years now her health has not been the best to say the least. She was in hospital recently and it looks like the simfastation was the problem. Her doctor lowerd her dose. I became suspiciuse and read a large amount of articals on choles trial and simvastatin and its side effects. Being a diebectic raises the chances of side effects. She has decided to come of the drug altogether now and feels a lot better. We put her ill health down to diebeties. Talking over her health over the last 8 years and the simtoms she has had apears to be with the drug rather than her diabeties
regards
Roy mcgly
Having read your article and the posts, I find it very informative.
It however, still seems as though higher lipid count is more negative than positive since the possible reasons therefore are contemplated. Does it therefore follow that there is a level that is ‘unacceptable’, or is it merely that this is the precaution your body takes and that whatever level it reaches, will be okay because your body produced it to function properly?
It would be interesting to know if every person has it’s own level of what ‘high’ or ‘low’ would constitute?
There is furthermore the concept of ‘inherited’ cholesterol, which seems to indicate that the person has higher than normal levels due to an inherited count from a mother or father and they then talk of ‘double cholesterol’. Could this be true, because that will indicate that it could not possibly be a natural process that took place in one’s own body due to natural requirements of the body itself?
Thank you for the informative articles and clear referencing.
Hi Rayno? Not sure which bit is first name/second name :-)
You raise some interesting points. This can be seen in a number of ways – the graphs in this post confirm that higher cholesterol is associated with lower deaths – that’s a vote for higher cholesterol. However – you are right to connect with possible reasons for high cholesterol. There can be many and they are by no means all bad and cholesterol is always the marker and not the cause of anything. e.g. a pregnant woman needs high cholesterol to make a healthy baby. Cholesterol should rise after surgery or injury to repair the body. The fact that the person has needed an operation or been injured is not good but the fact that cholesterol has risen to heal is good.
The only scenario I can think of where high cholesterol would be a bad sign would be with a high carb diet – we know that carbs impact VLDL – one of the components of total cholesterol. In this case the cholesterol would still be a marker – not bad per se – but it would be a marker of a bad diet, which will harm the person in the medium to long term.
With Familial Hypercholesterolemia (FH) (inherited) – which only genuinely affects c. 1 in 500 people and yet 1 in 8 people take statins – again – cholesterol is just a marker. With cholesterol in double figures (UK measures e.g. 13 mmol/l) – this would indicate that the LDL receptors on cells are not working properly (the definition of FH) and so the LDL lipoproteins are left in the blood stream. It is the fact that the goodies in the LDL ‘carrier’ are not able to get to the cells that will harm the person. The LDL in the blood stream is simply confirming that the receptors are not working properly. So idiot doctors then administer statins making it even more difficult for the FH sufferer to get the vital components of lipoproteins into the cell.
Hope this helps!
Very best wishes – Zoe
Hi,
I have a doctor’s appointment tomorrow and I know he will be pressuring me to take statins again. I am 60, low side of normal weight but not thin, average to low blood pressure (110/70), walk my dogs everyday but have high ‘lipids’. I am thinking of taking the prescription but not filling it just to get him off my case. Have to go in for something else. Not so easy to change your doctor here in Canada. Your work is reassuring.
Linda
Hi Linda – it’s not easy to change docs in the UK either – even harder to change their minds! ;-)
You may also find this one on statins interesting: https://www.zoeharcombe.com/2013/10/how-statin-drugs-really-lower-cholesterol-and-kill-you-one-cell-at-a-time/
You sound very healthy from your weight, BP and lifestyle (walking and dogs being the perfect stress managers) I bet your lipids are not even genuinely high – everyone has been redefined as high because the drug companies have lowered the targets. You’ll enjoy all of this but watch from just around 36 mins in if you’re short of time: https://www.youtube.com/watch?v=3vr-c8GeT34
Very best wishes – Zoe
Hi again Zoe. Thanks for the reply. I don’t know where you find the time to answer all these posts but all credit to you for doing so.
Thank you for putting me in the young section of old people. lol.
The 20% margin is interesting. Yes I did fast on both of these tests 12 hrs as requested? The vitamin D is worth thinking about although I have always had plenty of tuna and skimmed milk powder and now eat a tin of wild salmon most days. Sunshine, I love it I’ve always worked outside and the shirt comes off with the first rays.
The blockages, unfortunately are in the carotid artery in my head so there is no chance of stents (“according to the “specialist” £££?) Hence my interest in removing the plaque in a natural way??? I’ve done a lot of research into how and why the build up occurs. And I have read pretty much all of your links (thank you so much)
Stress, Mmm possibly? Processed Sugar, definitely no! My no no’s are anything that involves flour, (bread, pizza’s, cakes etc) and almost anything that involves processing. Ham, spam, burgers etc
McDonald’s UUGH! How any sane human being can put this muck into his or her body amazes me. I have taken on board your points regarding carb sugars and you may have ended up with another convert?
Exercise I am no triathlete. This would certainly put me in A&E. I do a bit of weight training, golf, tai chi, chi gong, stretching etc. treadmill for aerobics keeping a max bpm of about 150, spiking occasionally to around 160.
Aspirin. I was advised to take aspirin daily but it was giving me stomach problems so I starting eating lots of various fruits. Grapes, Dates, raisins, etc as snacks The idea was to increase my salicylate consumption and in doing so I would thin the blood naturally but due to getting headaches I have cut back on this practice, I believed that it was probably due to the salicylates? The headaches have now ceased. I am going to take half of one aspirin and see how it goes?
According to all my tests and I have had many, my heart, arteries, veins, blood flow and lungs are all in excellent condition. If my cholesterol is low how can I raise it and what should I be aiming for? Could you imagine the headlines. WONDER PILL FOR RAISING CHOLESTEROL.
Thanks once more Zoe, I am reading through many of your internet pages but it doesn’t get any less confusing, however keep up the good work. Pete.
Hi again Pete – you are not the first person to wonder why there is nothing to raise cholesterol! It is that good. I believe that – left alone – the body will make what it needs. You could artificially try to raise it by raising triglcerides with carbs – but you know that’s not a good idea!
Try this on stents: http://drmalcolmkendrick.org/2012/04/13/the-joy-of-coronary-arteries-the-body-aint-that-simple/
You sound in terrific health and your food and exercise choices seem ideal. There is a whole area of research into calcification and arteries. Malcolm would know about that. Vitamin K is the natural blood clotting assistant so it may be that you want less green leafy veg rather than more fruit? Not sure how the fruit would have helped.
Enjoy the reading!
Very best wishes – Zoe
Hi Zoe. Like many others I have found your articles interesting, informative and well documented. I especially like the fact that you are taking the trouble to answer many of the posts and hope that mine also would be included.
My story. Male age 66 extremely fit and active weight 140LLBS waist 33” chest 42” non smoker. Many years ago during days of heavy physical work and also exercise sessions I developed atrial fibrillation, (slight problem with my electrics). After many tests I was told to take beta blockers. I evaded taking them for many years by simply monitoring my heart rate and rhythms, cutting out salt and sticking to a good diet. Eventually though, through having arrhythmias I had to take them and now only take the smallest dose once a day (even though I am prescribed 2 a day) with no further problems and, I can work out with no discomfort (Obviously monitoring heart rate carefully). About 2+ years ago I started getting dizzy spells when I overdid work or exercises and ended up taking more tests only to find that I had 2 partially blocked arteries. All stringent tests/scans found no other problems.
Cutting a very long story as short as I can, I was told by my GP to start taking statins. Over past years I have always considered my diet to be excellent. I have always been involved and interested in good health and nutrition and due to this I had a little knowledge of what statins are and why I should not take them. (Previous tests have proved my HDL, LDL and triglyceride levels to be good) I asked my doctor why she was prescribing statins and she told me in a quite nonchalant manner that I needed to reduce my cholesterol? Being the type of person that I am I insisted on speaking to a specialist on the matter, an appointment was made. The meeting with the specialist went exactly the same way as with the doctor and with the same nonchalant manner. I asked the specialist whether there were any alternatives and he categorically stated NO. I then booked in an appointment for a cholesterol check.
Results as follows. (Fasting sample) 28th May 2013.
Total cholesterol/HDL ratios should be interpreted in relation to other coronary risk factors (including BP, diabetes, smoking, age, gender, triglycerides and personal and family history) please refer to Joint British Societies coronary risk prediction charts which are represented in the BNF.
Serum cholesterol 4.3mmol/L… serum HDL cholesterol level 1.2mmol/L… Total cholesterol HDL ratio 3.6… Serum triglycerides 0.9mmol/L…
Calculated LDL cholesterol level 2.7mmol/L. calculated using the friedwald formula
I recently had another blood test 3 April 2014. Showing a slight increase in all levels. Why I have the increase, I don’t know? I do eat a lot more fish now (tinned salmon)
Serum cholesterol 5.6… Serum HDL 1.6…Total cholesterol 3.5… Total triglycerides 1.0mmol/L. Calculated LDL 3.55 One concern was that my bilirubin level had increased from20umol/L to 35umol/L and this will be tested again in 3 weeks.
I have never had much faith in your average doctor I believe that most of them are just pill pushers and simply look forward to their pay packet at the end of the week. Most I’ve met are overweight individuals that know nothing about nutrition. And very little about the human body.
I have a question. I am hoping that, by eating the right foods and exercising to the extent that I am pushing my blood faster and with more pressure around my system I will eventually clear away some of the blockage in the arteries? Does this make any sense Many thanks Pete.
Hi Pete – so sorry I missed this one – been a busy week! You seem in absolutely tip top health – great waist/chest measurements and non smoking is always the single best avoidable thing.
Both of your cholesterol readings were low. Cholesterol is particularly protective in older people and old people – you fall into older ;-) Mortality studies for older/old people indicate that low cholesterol is the last thing you want. The graphs in this post clearly show it’s not just for this section of the population, but for everyone, that low cholesterol is not good.
Why was your reading higher the second time? There’s a 20% margin of error in the test – even before all the guessing that you’re aware of using Friedwald. This level of inaccuracy is known but rarely shared with patients. We had some nice weather early last year – you could have had some vitamin D? I doubt you’ve had much so far this year. Did you fast before the April 2014 test? Not that any of this is relevant – both readings are low and well within known margins for error.
The blockage one is heading out of my area of interest. What I can share is the general blockage process – https://www.zoeharcombe.com/the-knowledge/fat-does-not-clog-up-our-arteries/ – something causes damage and build up over the ‘scab’ can occur. You don’t smoke. You would be unlikely to be in such good shape eating sugar. So stress? What kind of exercise do you do? Is it what I would call unnatural?! You could be stressing the body with extreme exercise, in which case more would make it worse, not better. I’d go and see an open minded doctor (Dr Malcolm Kendrick is seeing people privately now, such is the demand for someone who doesn’t statinate – check drmalcolmkendrick.org) and investigate options. It could be as simple as aspirin for the anti-inflammatory effect or calcium build up may be worth investigating. Either way – statins will make your chance of repair worse, not better. In 4 years time you’ll be able to wave the patient leaflet at the doctor and point out that over 70 years olds should not be on statins. Doc won’t know that!
Good luck
Very best wishes – Zoe
Zoe, thank you so much for this info. It makes sense a lot. What I am trying to understand is since high level of cholesterol is a symptom of metabolic disorder why people could have normal cholesterol levels and get their arteries clogged.
Thank you.
Tatiana
Hi Tatiana – keep challenging! Who says high cholesterol is a symptom of metabolic disorder/risk factor? The same people who think cholesterol is bad and statins are good. Cholesterol is not bad in my world (or that of many other people). I do think that it is a marker. It can tell us about vitamin D levels (cholesterol is high when vitamin D is low because cholesterol turns into vitamin D with sunshine exposure). Higher cholesterol can mean the time of the year, it can mean a woman is pregnant, it can mean the person is injured/stressed/post an operation – any other factor which would lead the body to make more cholesterol. It can tell us many things but I don’t think it’s bad per se.
Try looking at a couple of the “myths & facts” down the right hand side – the fat, arteries and cholesterol ones especially. Damage to arterial walls (sugar, smoking, stress etc) causes lipids (including cholesterol) to be sent to the scene of the damage to repair that damage. One of the myths & facts explains how build up occurs and arteries can get clogged. Cholesterol is just trying to help!
Very best wishes – Zoe
Thank you for an informative article. I have copied it and will present to my GP.
I have just been diagnosed with high cholesterol, and been put medication to lower it. I have also been told to change my eating habits etc. My cholesterol level is 8.6, and based on my age of 67 the GP told me I had a 30% greater chance of a stroke or heart attack in the next ten years. This information was all on my local GP’s computer, which appears to have a program that churns out an answer once the results of the blood test are put in. I can only surmise that this is a standard ‘program’ for GPs, provided by the NHS. Therefore ‘high cholesterol is bad’ is set in stone.
I have to assume that I have a 30% higher chance chance than someone with low cholesterol levels? I asked if this meant that if I got my cholesterol level to zero, would I live another ten years? He didn’t think this was very clever.
I quote from your article “Back to – this is serious. Why are we lowering cholesterol when lower cholesterol is associated with more deaths from heart disease and all causes for men and women?”
This is ‘confirmed’ whenever someone receiving treatment for high cholesterol dies of a stroke or heart attack. Obviously, the damage was done by the cholesterol in the blood BEFORE the treatment started. Those who have never been tested (or treated) all died from other causes
Hi Nick – I laughed out loud at your question – brilliant! A couple of docs have looked at that computer game they’re playing with.
Here’s Dr Malcolm Kendrick: http://drmalcolmkendrick.org/2013/11/18/you-need-a-statin-now-what-was-the-question/
And Dr John Briffa’s: http://www.drbriffa.com/2014/03/07/how-good-is-the-tool-doctors-use-to-predict-who-should-be-treated-with-statins/
Everything on these sites is brilliant – this you may enjoy too:
http://www.drbriffa.com/2014/01/31/statins-associated-with-increased-risk-of-death-in-those-with-heart-failure/
You should also check your patient leaflet – the ones I’ve looked at for statins say not for those over 70 so you can ask doc why he is putting you on them for at this age anyway?! Or does he think he’s saving your life for 3 years despite the evidence for 192 countries?!
There’s also this – even more serious: https://www.zoeharcombe.com/2013/10/how-statin-drugs-really-lower-cholesterol-and-kill-you-one-cell-at-a-time/
Keep reading and suggest your doc does the same :-)
Very best wishes – Zoe
Same to you Zoë. Listening to your Youtube-films and wondering how to give a punch to the old wrong establishment of healt and a kick some where at the rear. Feel free to use my e-mail.
Hi. One of the Swedish gold medalist at the latest Olympics in Sochi is a LCHF – Low Carb High Fat athlete. Only different he have seen is that he lost some more fat on his body. No different in energy. Björn Ferry is his name.
Hi Micke – many thanks for this. We like to keep examples like this for amateur athletes who are trying to move away from carb loading
Best wishes – Zoe
I’m 50yrs old, and I just had “the widow maker” heart attack 6 days ago, but was fortunate to be living within a 5 minute drive from a very good hospital. I have a history of heart disease on my dad’s side of the family. Long story short, I was told (not shown) that my cholesterol levels are “normal” (no one showed me any numbers on any tests). My demigod doctor showed op on my third day in the hospital and thought he would practice his bedside manner. (He failed). He started out talking about how I need to change my diet (he never asked me what my diet is), and I mentioned that the tie between dietary cholesterol and heart blockage is not very strong (I was going by memory, remembering the British study with 20,000 participants over a decade called Mr Fit). Instead of going on and talking about how compromised my heart is, what the “echo” tests have shown, etc or what I can expect in the future, he LITERALLY pointed his finger at me and said “I’m right and you’re wrong, and you believing that nonsense us like you not believing in gravity”. He left soon after that, with a parting comment that I need to start “believing in gravity”. I gave him a pleasant lip-smile the whole time, but I’m going to request a different doctor, obviously, as he might be very technically skilled and learned surgeon, but he’s unscientific and unprofessional. (Since when does science have anything to do with personal belief?)
I’ve worked with “Dr’s” (medical and non-medical) in several different fields in my life, and I’m always struck dumb by the degree of arrogance the vast majority of them tend to have.
Hi JM
I’m so sorry to hear about your recent attack and just as sorry to hear about your ‘patient’ experience. Good luck with your recovery and finding a nicer doc!
Best wishes – Zoe
Hi Zoe, thank you for this very interesting article.
I know you specialise in the obesity side of nutrition, but what are your thoughts for athletes, that actually require higher levels of energy and find carbohydrates as a useful source? Due to the nature of high GI foods, athletes tend to turn to these during physical activity, in order to replenish glycogen stores faster and also provide the body with readily available energy in the bloodstream. It’s actually quite hard to expect athletes to not have a high carbohydrate diet. Obviously athletes would be considered as healthy individuals and are less prone to diseases but surely based on what you mention in this article, the “fast releasing” carbohydrates may still cause damage to vessel walls and in turn increase LDL levels.
Thanks,
Alex
Hi Alex
I could debate this one!
One thought is that it depends on the exercise being done. There may well be an argument for unnatural activity (marathons, iron man stuff, long cycle rides etc) needing unnatural fuel (carb loading). Normal activity (walking, working as a labourer, gardening etc) should not need any carb loading.
Having said this – I can also see an argument that not even unnatural activity requires carb loading and there is certainly an argument that the better tuned an athlete is to burning fat, the more competitive advantage they can acquire.
You’re right that I’m more interested in the obesity side, but I have worked with a couple of professional athletes and a few ‘amateur’ athletes (if doing even one leg of the tour de France is amateur!) to help them with weight and performance. Carb loading doesn’t help weight so an athlete needing optimal power to weight ratio can benefit from dropping carb intake to reduce weight. This needs to be achieved with no loss in performance and it can be done – but my sample sizes are very small.
I would point you in other directions for more evidence:
– http://www.mensjournal.com/health-fitness/nutrition/paleos-latest-converts-20130618
– http://thelowcarbdiabetic.blogspot.co.uk/2013/12/australian-cricket-team-thrash-england.html
– http://www.marksdailyapple.com/a-metabolic-paradigm-shift-fat-carbs-human-body-metabolism/
Check out Djokovic going gluten free and many more professional athletes are not carb loading for optimal performance.
Thinking about it – the body will always use glucose if available – in the blood stream and then stored glycogen. The max energy we can store as glucose/glycogen is c. 2,000 cals in the extreme – many people far less than this. I’m 110lb and less than 20% body fat, but that still means I’ve got c. 20lb of fat to live off. The 3,500 calorie theory is not accurate, so it’s not as simple as saying I have 70,000 calories available (and I don’t want fat around organs lost) but you can see how training your body to burn fat would be a far better idea than training it to burn carbs!
Research low carb athletes – there’s a whole world out there of people munching butter and not fake energy drinks, bars and gels – and they’re doing very nicely.
I’ll stick to gardening and walking the dog!
Very best wishes – Zoe
“Why are we lowering cholesterol when lower cholesterol is associated with more deaths from heart disease and all causes for men and women?”
Because low cholesterol is a marker for a variety of health problems/diseases/etc. such as cancer, frailty syndrome etc. etc. Lowering elevated LDL via diet, exercise, medication etc. etc. doesn’t increase CVD or all cause mortality.
That wasn’t so hard, now was it?
My mother in law is healthy as a horse. She’s 92 years old and she had high cholesterol all her life. They put her on Lipitor in her 80’s. I have no idea why because she doesn’t have heart disease, but she does have dementia now. (not sure if related to drug)
My mom has heart disease, she also has high cholesterol. She is 89 and healthy other than the CVD. My dad DID NOT have high cholesterol and he had heart disease. He was also on Lipitor. BTW NOBODY HAS HAD CANCER. This is all antedotal of course.
Please provide scientific study that says high LDL causes cancer. (no observational studies please) Also please provide scientific study that says meditation decreases LDL.
Thanks for doing this research and proving what I suspected. I lost 70kg (over 150lbs) following my own diet … I never avoided animal fats .. rather included the right amount of animal protein (including lots of eggs) with mostly fresh vegetables, a few complex grains, nuts and a little fruit. My total cholestrol was never high, even when I weighed over 143kg it sat around 3.8, but on my ‘diet’ it dropped to 2.0. I just don’t get the meds thing. The body has a way of working iteself out if you put the right stuff into it … and yes that means no sugar or highly processed foods. It’s done this for thousands of years and will continue to do so, only if we let it.
*saturated fats! not “attracted” fats. (Curse autocorrect)
Great piece of work. One note though on dietary saturated fat raising cholesterol. Yes, the cholesterol in LDL is related to consumption of carbohydrates, but I have read from several sources the assertion that some saturated fats down regulate the uptake of LDL particles by the liver, with the indirect effect of raising LDL levels by causing more LDL particles to circulate in the bloodstream longer. Assuming oxidation of LDL as atherogenic, then this would increase the amount of oxy-LDL in the bloodstream. Presumably other aspects of more saturated fat offsets this, given the lack of correlation of saturated fat to actual CVD. Nonetheless, it may be misrepresentative to say that attracted fats do not affect levels of LDL.
i have lost 6.5 stones over last 2 year by trying to follow the zoe diet and still need to drop 2 more stone ,iv never felt better in my live.i do 7miles walk once or twice a week.plus zumbra twice aweek.which i didnt do anything before. i do get checks by my doctor and is very happy with
me so far.