
Cholesterol & heart disease – there is a relationship, but it’s not what you think
This post is dedicated to Anne who asked me a great question about cholesterol. It made me do what I had been meaning to do ever since I read Dr Malcolm Kendrick’s The Great Cholesterol Con…
Dr MK ran some analysis on World Health Organisation (WHO) data. The WHO has extensive data from almost 200 countries on more health measures than you could imagine – definitely worth a look one rainy, wintry afternoon. This is where Dr MK presented the world with two different Seven Country Studies – (for those of you who aren’t familiar with the history, it was the Ancel Keys’ Seven Countries Study that started all the fat heart hypothesis stuff). Dr MK took the seven countries with the lowest saturated fat intake and then the seven countries with the highest saturated fat intake. You may need to read this twice – but he found: “Every single one of the seven countries with the lowest saturated fat consumption has significantly higher rates of heart disease than every single one of the countries with the highest saturated fat consumption.”
The next chapter in The Great Cholesterol Con goes on to look at cholesterol and heart disease (and overall death rates) and quotes many great studies where it is shown that lower cholesterol is associated with higher mortality. However, it did leave me thinking – having run the data on saturated fat and heart disease, let’s just run all the data on the cholesterol and heart disease and get to the bottom of this hypothesis from all parts of the allegations.
It actually didn’t take that long – less than a couple of hours one Saturday afternoon. You go to the WHO statistics area of their web site and then pick data for cholesterol from risk factors (how judgemental to start with!) and then look under: Global burden of disease (mortality); All causes; Non communicable diseases and then G Cardiovascular disease (shortened to CVD). CVD deaths include ischemic heart disease and cerebrovascular disease – that means fatal heart attacks and fatal strokes to us. You find the most recent year where you can get both sets of data to compare like with like. This turns out to be 2002. You download their very user friendly spreadsheet data (CSV) – cut and paste it into an excel file and then try to remember how the heck to do scatter diagrams in excel!
Before telling you the results, we need to go back for a quick reminder on what we know about cholesterol and then hopefully this can serve as a factsheet for all the cholesterol questions we continually get.
The role of cholesterol
It is virtually impossible to explain how vital cholesterol is to the human body. If you had no cholesterol in your body you would be dead. Every single cell of your body is covered by a membrane (think of a membrane as the ‘skin’ or protective barrier around each cell). This membrane is made largely of cholesterol, fat and protein. Membranes are porous structures, not solid walls, letting nutrients and hormones in while keeping waste and toxins out. If cholesterol were removed from cell membranes they would literally explode from their internal water pressure. Human beings quite simply die without cholesterol.
Cholesterol is vital for hormone production – the sex hormones and therefore the entire human reproductive system are totally dependent on cholesterol. Hence, not only would humans die without cholesterol, the human race would die out.
Cholesterol is vital for digestion. The human body uses cholesterol to synthesise bile acids. Without cholesterol-rich, bile salts, the human body could not absorb essential fatty acids or the fat soluble vitamins (A, D, E and K) and serious, even life threatening, deficiencies could develop. (It is interesting, therefore, that nature puts cholesterol in virtually every food that contains fat – providing a digestion mechanism in tandem).
Cholesterol is vital for the brain, central nervous system and memory functions (hence how the side effects of statins include memory loss, mental confusion and people generally just not feeling themselves). Even though the brain is only 2% of the body’s weight, it contains approximately 25% of the body’s cholesterol. The vital connections between nerve endings in the brain, which help to conduct the electrical impulses that make movement, sensation, thinking, learning, and remembering possible, are largely made up of cholesterol.
Cholesterol is critical for bones and for all the roles performed by vitamin D. Vitamin D is best known for its role in calcium and phosphorus metabolism, and thus bone health, but we are continually learning more about potential additional health benefits of vitamin D from mental health to immune health. Vitamin D can be ingested (and is, interestingly again, found in foods high in cholesterol) and it can be made from skin cholesterol. Modern ‘health’ advice to avoid the sun, take cholesterol-lowering drugs, eat a low cholesterol diet (whatever the heck that is supposed to be) – combined with there not even being a recommended dietary allowance for vitamin D – is undoubtedly contributing to avoidable modern illness.
One of the key reasons that we need to spend approximately one third of our lives sleeping is to give the body time to produce cholesterol, repair cells and perform other essential maintenance.
This gives you the headlines of the vital functions that cholesterol performs, but hang on to that bottom line – it is utterly vital and we die instantly without it.
You may be familiar with the term essential fatty acids or essential amino acids (proteins break down into amino acids). The term ‘essential’ used like this in nutrition means that it is essential that we consume it in our diet because the body can’t make it. The body makes cholesterol. That says to me that cholesterol is even more vital than essential fatty acids or essential amino acids – even though these too are life critical – and therefore the design of the human body is such that it was not left to chance that we needed to get cholesterol from food. Of the 500 or so roles that the liver has – one is to produce cholesterol. It is too vital to be left to chance.
What went wrong?
So, how did something so life vital become more vilified than a mass murderer? I think it comes down to three things (and I don’t take credit for this view – it is there to be worked out by anyone who traces back the history and Kendrick, Uffe Ravnskov and all the thincs.org guys have led the way):
1) Rabbits;
2) Ancel Keys;
3) Money!
1) In 1913, a Russian chap called Nikolai Anitschkow decided to feed rabbits purified cholesterol and he managed to get their blood cholesterol levels in excess of 1,000 mg/dl (nearly 26 mmol/L! Most UK people have levels of 5-7 mmol/L). He then noticed the formation of “vascular lesions closely resembling those of human atherosclerosis” forming in the arteries of the rabbits. The obvious flaw in the experiment should have been that rabbits are strict herbivores. They do not eat animal products, which is the only source of cholesterol. Hence rabbits are in no way designed to digest cholesterol or animal fat and no one should be surprised if cholesterol or animal fat ended up stuck in any part of the poor rabbit. The only surprise is that no one thought to ask Anitschkow why he was feeding cholesterol and animal fat to herbivores. Interestingly, far less well known is that a parallel test was done on rats and dogs (omnivores) and feeding cholesterol to these species failed to produce lesions.
2) Ancel Keys. Remember the Minnesota experiment that I so often refer to? A brilliant and unbiased piece of research, which has given the world one of the best insights into low calorie dieting ever done – it was pure genius. This study made Ancel Keys the man of the moment and I guess he wanted to follow it with something equally impactful. There is an anecdote in The Great Cholesterol Con and on p113 of The Obesity Epidemic where Henry Blackburn, one of Keys’ closest colleagues, tries to explain what may have fuelled Keys drive to find a connection between diet and heart disease.
What is little known is that Keys originally tried to establish a link between cholesterol in food and cholesterol in the blood (our cholesterol levels when we have a blood test) because he thought (probably because of poor Bugs Bunny) that cholesterol in the blood causes heart disease.
Keys did multiples of studies, changing the diets of his human ‘guinea pigs’, and he presented his conclusions in The Journal of Nutrition, November 1955: “It is concluded that in adult men the serum cholesterol level is essentially independent of the cholesterol intake over the whole range of natural human diets. It is probable that infants, children and women are similar.” i.e. I only tested adult men and there is no relationship between cholesterol eaten and cholesterol in the blood and it is probable that there will similarly be no relationship for women or children.
In 1997 Keys put this even more assertively: “There’s no connection whatsoever between cholesterol in food and cholesterol in blood. And we’ve known that all along. Cholesterol in the diet doesn’t matter at all unless you happen to be a chicken or a rabbit.”
Did you know – even the UK Food Standards Agency (FSA) and UK National Health Service (NHS) admit this?
– “However, dietary cholesterol has little effect on blood cholesterol. More important is the amount of saturated fat in your diet”. (National Health Service). (Notice the second sentence? They just couldn’t let the theory go).
– “But the cholesterol we get from our food has much less effect on the level of cholesterol in our blood than the amount of saturated fat we eat”. (Food Standards Agency). (This link may disappear, as the FSA is bowing out of giving nutritional advice).
What the government advice should say is: The body makes cholesterol. The cholesterol you eat has no impact on the level of cholesterol in your blood – not “little”, but “no” – (and we’ve known that all along). And they should also explain how saturated fat can determine blood cholesterol levels and then provide irrefutable evidence that it does. But it must be hard for public health bodies to even go this far. As we saw in a recent thread – the FSA also now accept that there is no limit on the number of eggs we can eat: 
If only Keys had stopped here, but he wanted to find an explanation for heart disease and he was not about to be deterred. For some reason, which I find inexplicable, he then turned to fat (the entire literature on this topic is very vague about “fat” vs. “saturated fat” so his early writings are also very vague on the topic). Here’s a bit of Mensa logic for those who like this kind of thing:
i) Only animal foods contain cholesterol (meat, fish, eggs, dairy). NO non animal foods contain cholesterol.
ii) All animal foods contain fat – saturated and unsaturated. Some may be very low in fat (e.g. white fish), but they all contain some fat.
iii) If there is no link whatsoever between increased consumption of foods containing cholesterol and blood cholesterol levels, there can be no link whatsoever between increased consumption of animal foods and blood cholesterol levels since only animal foods can be increased in consumption to increase consumption of cholesterol!
So, Keys first did the graph that was presented at the Mount Sinai hospital (which is the one shown in the Tom Naughton video and in Dr Robert Lustig’s “Sugar: The Bitter Truth” ) and then went on to do the Seven Countries study – which I have read all twenty volumes of and take apart piece by piece in Chapter Eight of The Obesity Epidemic: What caused it? How can we stop it (on this page).
As Kendrick’s two unbiased seven country studies showed – there is not even an association between saturated fat and heart disease – let alone a causation. However, Keys published his seven countries study and the rest, as they say, is history.
3) The Robert Redford film All the Presidents’ Men that had the memorable quote “follow the money”. This is absolutely at the heart of everything in the diet industry from national dietary organisations to the food, drink and drug industries and individuals in between.
The Ancel Keys work interestingly claimed that saturated fat consumption (A) caused heart disease (C) not directly, but by raising cholesterol (B). Hence A was supposed to cause C through B. For this to even get off the starting blocks, A and C have to be related (plot one against the other and there has to be a clear relationship); A and B have to be related and B and C have to be related. None of these in fact holds. The Kendrick study shows that A and C are not related. There is no logic that A and B could be related – because of the problem of fat and cholesterol being found in the same foods and Kendrick presented many studies that showed B and C were not related. I aim in this article to put the nail in the coffin for any idea that high cholesterol is even associated with high heart disease. We will, in fact, show that the evidence confirms the opposite.
By having cholesterol as this middle-man, this has allowed an entire pharmaceutical industry (and stupid cook books) to come up with ways of lowering cholesterol. The most lucrative of these has clearly been statins – drugs designed to stop the body producing the cholesterol that it is designed to produce. It never hurts to remind people that one statin alone, Lipitor, has been worth $125 billion to Pfizer since 1997. Taubes has a deeply troubling passage in The Diet Delusion where he looked at the committee who approved a lowering of the target cholesterol levels for the USA population. From memory (it’s a big book to find a reference!), a number of people were on the committee and all but one were funded by pharma companies and one didn’t want the target cholesterol level lowered. I wonder which one! (Anyone reading this – if you can find the page number I’d be so grateful – my copy has so many scribbles on I can barely read it).
So, cholesterol will remain the mass murderer for as long as statins are as lucrative as they are or until the public are enlightened and courageous enough to say no to doctors who try to put them on this medication (like my mum was after reading Dr MK!)
A small technicality
On p35 of The Great Cholesterol Con, Kendrick says: “How can eating saturated fat raise LDL levels? It is not merely biologically implausible, it is biologically impossible. Boy does that statement make me a hostage to fortune!”
I arranged to meet a biochemist at a local university to try to get to the bottom of this statement. The biochemist (who has more qualifications than I’ve had dark chocolate) was sadly so brainwashed in the ‘fat is bad’ theory that he just kept saying eating fat raises cholesterol. When I asked him to talk me through the biochemical pathway from fat digestion through to how this impacts cholesterol he said he didn’t know the digestive process well enough – we would need to add a dietician into the conversation. This was alarming enough. I then said – we eat 39 grams of butter per person per week in the UK and about 1.4 kilos of flour – didn’t he think it was more likely that the flour was making us fat and sick. He said it only took a drop of arsenic to kill us. I left shortly afterwards.
Kendrick has to be right (isn’t he always?) LDL (remember this is not cholesterol – it is a low density lipoprotein) is the left over from IDL (intermediate density lipoprotein), which is the left over from VLDL (very low density lipoprotein). VLDL is one of the measures you get in your blood cholesterol test (actually they estimate it – they don’t measure it – they only measure total cholesterol and HDL leaving two other unknowns in an equation with four variables and you thought this was scientific). (They also call VLDL ‘triglyceride’, which is confusing and unhelpful). Cutting a complex story short (it is explained in my book in different passages), carbohydrates can impact VLDL levels (starter for 10: Acetyl-CoA being the start of the process by which the body makes cholesterol and part of the Kreb’s cycle whereby the body turns glucose into ATP), but I really have found no way in which the fat that we eat can do so. Because fat is not water soluble, it is packaged into a lipoprotein in the digestive system. The lipoprotein that fat goes into is the biggest one – the chylomicron – and then it travels off into the body to go and do the essential repair and maintenance jobs that fat does. Does the fat say – hang on Mr chylomicron – we need to go via the liver and see if we can mess up the body’s VLDL production in some way?! Do ask this ‘how’ question (in detail) of someone who thinks that this is possible. I am still open to someone answering this, but I’m not holding my breath.
Fructose, on the other hand, we do know goes straight to the liver to be metabolised. Could that, and other carbs, impact VLDL production? The evidence I have already seen is strong that they do.
The serious bit
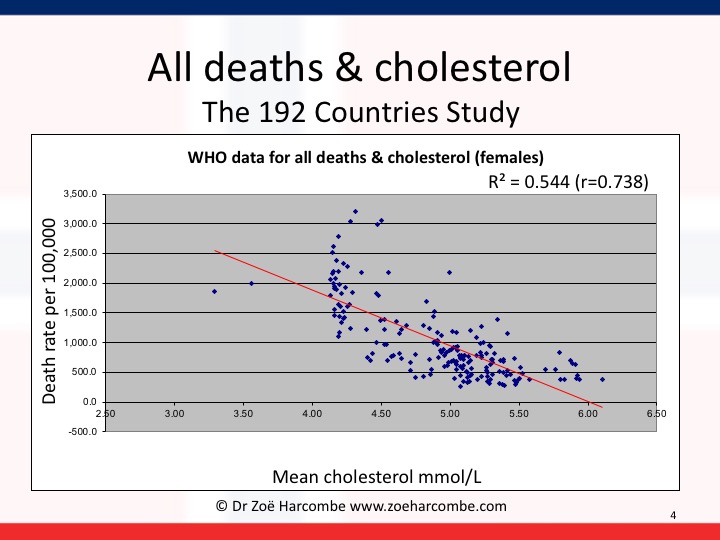
The WHO data is split into men and women. I first did the scatter diagrams for average (mean) cholesterol levels and CVD deaths. Then I ran the Pearson correlation coefficient on these numbers. This gives us the term called “r”. “r” tells us if there is some kind of a relationship: an r score of 0 would indicate no relationship; an r score of 1 would indicate a perfect relationship. A negative r score is called an inverse relationship e.g. the price of concert tickets is likely to be inversely related to the number of concert tickets bought – fewer tickets being bought at higher prices.
The “r” score for men revealed that there was a small relationship of 0.13 – however this relationship was inverse. The diagram and correlation shows that higher cholesterol levels are associated with lower CVD deaths and lower cholesterol levels are associated with higher CVD deaths. In women, the relationship is stronger – to the point of being meaningful. The r score was 0.52 – but, again, inverse. For women, higher cholesterol levels are quite significantly associated with lower CVD deaths and lower cholesterol levels are quite significantly associated with higher CVD deaths. Please note that I have added r squared on the graphs below (excel can do this for us) and it can confirm that you’ve got your r numbers right and r squared tells us the strength of any relationship we have observed.
All you need to do is to look at the lines going down to the right and wonder how on earth we ever got away with telling people that cholesterol causes heart disease. High cholesterol is associated with lower heart disease and vice versa – for all the data available in the world. High cholesterol is not even associated with high heart disease, let alone does it cause it.


It gets worse. I then kept the cholesterol information and changed the death rates to total deaths – all deaths from any cause – cancer, heart disease, diabetes, strokes – all deaths. You can see the diagrams for men and women again below. This time there is a significant relationship for both men and women: 0.66 for men and 0.74 for women – again inverse. There is a significant association between higher cholesterol levels and lower deaths and lower cholesterol levels and higher deaths for men and an even more significant relationship for women.


This is serious. I’ve shown it to a couple of academics (Professor sort of things) with whom I’ve been having great debates, as I want to see what the view is from people who wholly believe the fat/cholesterol/heart/death hypothesis. (Kendrick talks in his book about what happened when he showed an intelligent colleague his two seven countries studies and the evidence was just dismissed instantly). It is most useful to know what the resistance arguments will be before starting to invite the resistance. The two arguments I got back were:
1) “Ah yes – but this is only an association.”
Ah yes – but a) we changed global dietary advice back in 1977-1983 on the back of an association in Seven (carefully hand picked) Countries that miraculously became a causation even when the association was far from established and b) it is an association that’s the opposite to the one that the world currently holds true and c) that’s what epidemiology is supposed to be about – establish an association and then investigate if there could be any causation or useful learnings. So – go out with a new paradox – that high cholesterol is associated with low deaths and then see what dietary advice emerges.
2) “But that’s total cholesterol – the key thing is the ratio of good to bad cholesterol.”
Oh boy! The chemical formula for cholesterol is C27H46O. There is no good version or bad version. HDL and LDL are not even cholesterol, let alone good cholesterol or bad cholesterol. They are lipoproteins – see above – and they carry cholesterol, triglyceride, phospholipids and protein. Do you think that taxis are people? Or do you think that they are carriers of people (and luggage, and pets and fresh air and other things).
Back to – this is serious. Why are we lowering cholesterol when lower cholesterol is associated with more deaths from heart disease and all causes for men and women?
The doctors’ Hippocratic oath is “First do no harm”.
This also says to me – even though saturated fat has nothing to do with cholesterol, it doesn’t actually matter. Even if it did – cholesterol is only associated with CVD deaths in an inverse way. If fat did raise cholesterol – as public health officials like to claim – it could save lives! Please note I am always really careful with language in this area and never jump from association or relationship to causation. Someone may be in the bath and they may be singing – if we observe this in many cases, we may claim that there is an association. We cannot say that bathing causes singing or that singing causes bathing.
Our global dietary advice was changed in 1977 in the US and 1983 in the UK as a result of a biased study of seven handpicked counties. Had the data been available for the 192 countries we can analyse now, or had Keys even considered all the data that was available to him at the time (for France etc), our conclusion may have been that we need to protect cholesterol levels in the body. We may have realised that the last thing we should be trying to do is lowering cholesterol – unless we’re trying to lower life expectancy for some reason.
Zoë Harcombe



I believe the US Framingham study linked cholesterol with CHD, but careful reading of the study shows no association after age 50. Good discussion in Overdosed America by John Abramson.
Hi I have been looking at Dr Kendricks 27 factors and the scottish study that he gave a talk about. One criticism from the Cholesterol supporters is that it deals with all death and at first I thought OK but surely the factors equally apply to CHD and CHD death but looking at the original report at BMJ this does not appear to hold. Increased cholesterol means an increased hazard ratio for CHD, see data below
All CHD 1 1.13 2.05 2.15 3.15 1.34 (1.34 to 1.44) *** 1 2.43 2.97 3.51 3.94 1.28 (1.12 to 1.45) ***
CHD deaths 1 1.14 1.50 1.74 2.21 1.23 (1.09 to 1.38) *** 1 1.10 3.23 1.87 2.2
Anyone shed light on this
I love science…especially when the “facts” are manipulated to sell us all something. Global warming is a myth and I truly believe that this Cholesterol scam is also a myth. It just makes so much sense that if the body makes cholesterol, it must need it and in the quantity that it needs it. I also love the fact that for me, it is always better to exercise and eat a comfortable amount of food, get enough rest and not add to my problems. I quit all forms of smoking, cigs and cigars…I don’t inhale either…lol I had a heart attack within a year of quitting smoking. My cholesterol was just fine on a very low carb diet as was my blood pressure. Unfortunately, I allowed myself to get out-of-shape and gained a whole lot of weight. I listened to my Cardiologist and lost weight by reducing calories…on-going. I just had my Cholesterol checked and the overall number came down 5% and the LDL/HDL/Tri are all off of the dr’s chart…He wants a Statin…I don’t. The problem is this…until I started to get regular checks on Cholesterol, I never had it checked and now, I have nothing in my past to reference the numbers for my “normal”…I suggest a cholesterol check up from birth to old age to use as a guide…That way, each person can guage their normal and respond according to it and not to a Pharm company….
Don’t associate everything is a conspiracy with this article. Clearly there is financial incentive to corn oil, big pharma etc. However, Global warming is real. Proven with thousands of studies and overwhelming evidence and with “the money” being against it! You are witnessing it now. A radical jump in temperature and extreme weather that is unnatural! Next you will tell me the Bible is the word of God! lol
Perfect response JGS. People who force themselves to ignore the mountains of proof of global warming just don’t want it to be true for some reason. And anyone…who uses ellipses…like David…is a moron anyhow.
I think that David “meant” that HUMAN INDUCED GLOBAL WARMING is a MYTH when we all
KNOW it is actually a SCAM ! ( “Anthropogenic Global Warming” a la AL GORE ! )
“Climate Change ” is the new terminology BECAUSE the planet has ceased warming for at least the
last 10 years. “Climate Change” IS REAL….it is ALWAYS changing…….from cold to warm and then back to cold again. WE ARE STILL IN AN ICE AGE !!!
This is simply a warm interlude ( an inter- glacial ) with the maximum glaciation 22,000 years ago ,
another about 13,000 years ago and another about 11,700 years ago. Since then it has warmed up enough BY NATURAL CAUSES to allow 7.5 BILLION humans to exist with enough ice melted to expose the land we now live on and grow food on !
Thank your lucky stars you were born into such a clement environment ! Now use your talents
to at least GOOGLE “Last Glacial Period” (Wiki) and get some FACTUAL INFORMATION before making any more silly uncorroborated statements !
This is the KIND OF ILL-INFORMED BELIEF SYSTEM that Dr Harcombe is attempting to point out that
exists in the MEDICAL SPHERE to the detriment of all concerned.
EVIDENCE ! EVIDENCE ! EVIDENCE ! Don’t just quote people who write newspaper headlines or
want to sell wind-turbines or photovoltaic-power panels ! There has been NO radical jump in
temperature ! Storm and extreme weather events have LESSENED recently !
0.8 degrees Celcius increase in temperature SINCE 1850 up to now is NOT radical…..it is BARELY
MEASUREABLE ! Good grief ! The temperature between when you got out of bed and the temperature at lunchtime was probably 5 to 10 degrees in extent ! Did THAT feel extreme ? No !
Of course not ! Sea-level rise….imperceptible ! No islands have sunk….although Venice has been
on the verge for a thousand years ! ( Bad wooden foundations ) . ‘Isostatic Rebound’ or
Post-Glacial Rebound ( now the weight of ice has lifted off the crust ) is causing vast areas of land to
rise , in some parts of Scandinavia up to 1 metre ( 3 feet ) every 100 years , which more than matches Sea-level rise. Al Gore GOT MOST OF IT WRONG but it is proving very hard to overturn the
self-serving FALACIES and LIES HE PROMULGATED !
Once a FALSE BELIEF becomes “AN ESTABLISHED-TRUTH” it is hard to shake off EVEN when you can
PROVE IT WRONG WITH FACTS and EVIDENCE !
The same is true of the MEDICAL INDUSTRY and it will only change as the MORE RECENTLY
EDUCATED and better informed professionals take-over from the existing practitioners as they
retire and are replaced. However , it is a slow process and everyone would be well advised to learn
as much about their own body and biology and any diagnosed ailments as they can for their own
benefit.
We have had extreme weather conditions in the past. Check your resources. We definitely have climate change, but it is cyclical. The only scientists the media relies on are those that believe the world is ending!
Brilliant, Zoe – good old cognitive dissonance – may take a while for the penny to drop but drop it will
OKi see all the data Zoe presented. Please tell me about how blocked arteries get blocked, then leading to heart attacks?
Hi April
Many things can damage the arterial wall – stress, smoking, sugar, chemicals, pollution, some drugs, some medical conditions etc (check out drmalcolmkendrick.org for a brilliant review of what really causes heart disease)…
When damage occurs, a ‘lesion’ forms (think of a lesion as a ‘scab’). The body is so clever and self protective that the body cannot and does not risk the scab breaking away and freely floating in the blood stream – as this could cause a blockage. The lining of the endothelial wall tries to repair itself and forms a new layer over the scab – sucking the scab back into the lining of the artery wall in so doing. That’s how smart and life preserving our bodies are. The trouble is – if we continue to be exposed to whatever was damaging the lining of the arteries (smoking etc – see above) – we continue to form lesions. We only need too many ‘scabs’ in one area, and the repair kit being unable to keep up, and we could be in trouble – big heart attack or stroke kind of trouble.
That’s how arteries narrow and eventually become blocked. I could say that cholesterol has nothing to do with it, but cholesterol is one of the repair substances needed by the body, so cholesterol will be deposited at the scene of the damage to try to repair that damage. Cholesterol no more causes the damage than fire fighters start the fire – they’re there because it happened.
Best wishes – Zoe
2) “But that’s total cholesterol – the key thing is the ratio of good to bad cholesterol.”
Probably true, but doesn’t the low carb/high fat approach change these ratios in a positive way? i.e. High HDL/low Trigs.?
As a FORMER Angina patient I rejected the doctors advice to take SSRI (anxiety) to lower my blood pressure and a STATIN for high HDL… I only opted for an Asprin (which I now have replaced with Cayanne Pepper) and the “Nitro” pills as a emergency pain vasodialator.
I stopped most processed food (chemicals) and started high fiber, and inflammation lowering foods, such as garlic, lemon, spinach, beans, etc…..and I still eat meat and fats… the removal of the chemicals and this altered diet (to me Spicy Chili con Carne with beans is a superfood) I have been symptom free and not used a Nitro pill for 8 months, I played basketball yesterday, and last year I could not even walk up a flight of stairs.. NEVER TAKE STATINS or SSRI DRUGS !
Well done Michael, Try using Kyolic Aged Garlic. There was an interesting trial recently that showed that KAG stabalised and in some cases reduced evidence of arterial plaque. Link below
https://heartattackandthenhs.wordpress.com/2015/08/12/kyolic-garlic/
well done. there are two meta analysis one by turner and one by irving kirsch on ssri snri 3rd generation antidepressants. They are no more effective than placebo when you get all the studies the scum pharmaceutical companies fail to publish that are negative. Also seratonins mood boosting effects are mythical. Seratonin when injected is a sedative that causes helplessness and apathy, suicide is 3 fold higher using these. Once you have used them you are more likely to be depressed in the future, seratonin also can encourage aggression. Depressed people do not shoot up schools but depressed people with a history of antidepressants do. Seratonin causes hypertension as it is a coagulant and a vasoconstrictor it is also called thrombotonin due to this effect. It is a damage induced inflammation mediator, the behavior the drugs incur on plateletes ability to uptake seratonin is the same behavior seen performed by bacterial endotoxin and can be seen in people with alzheimers and ms. Animals in learned helplessness studies have high seratonin, these animals that would normally swim for hours stop swimming and drown in these studies. seratonin is also found to be high in those with autism and asthma, it enhances nitric oxide and prostaglandin 2 based inflammation worsening arthritis. seratonin is excitotoxic as it activates glycolysis leading to a build up of lactate inhibiting mitochondrial respiration which makes it carcinogenic. People take tryptophan supplements to boost seratonin this is just as dangerous and involves other metabolites that boost chances of cancer and diabetes. Tumors increase seratonin and help it to metastasize and proliferate hiding in clots and leading to the 2nd leading cause of death in those with cancer in hypercoagulation. Drug companies are full of marketing spin about seratonin and it has become a popular myth that it boosts mood, actually other antidepressants exist that lower seratonin, these might actually work. Why did this idea that seratonin would be beneficial originate, because governments spread propaganda about LSD which is antiseratonigenic and causes playfulness. If you look up bromocriptine the disorders this is used for also have high seratonin factors, being an antiseratonigenic, ashwaganda is also one. The only reason 3rd generation antidepressants exist is due to the other generation patents expiration, they simply dont work other than to do harm. They never could have as the substances physiology is contraindicated.
Unfortunately data is for mortality rates and doesn’t account for intervention rates that are greatly variable in success rates in different countries I’d imagine. Are there databases dealing with incidence of disease as opposed to mortality?
Thank you!! I knew there had to be “something” in there and your comment could pretty much answer that.
I see exactly where you’re coming from, if doctors are telling people to lower their cholesterol then there are less people out there ignoring the signs and having a heart attack as a result!
For this to be an accurate study they would have had to take an equal amount of people from each cholesterol level and compare the heart attack rates.
perhaps the people up at 6.0 don’t have many because a lot of them are already dead before they get there?
I also note that cholesterol levels of 4 or below have hardly any dots… is this also saying something?
Good point.
This is, as the teens here say, A.W.E.S.O.M.E. I’m saving this. Love your work. Please keep it up.
Pingback: Destroying the recent statement from the Heart Foundation | The Big Fat Truth
Hi Zoe,
As I am not as knowledgeable about this issue perhaps you could answer a q or 2 please?
I am 29 and have been on cholesterol medication since I was 18. Without it my cholesterol reaches between 10-12 mmol
There is no heart attack/stroke history in my family even though my high cholesterol is a genetic thing that all my family have.
I live an active healthy lifestyle with a paleo diet. In the past I have found when I have stopped taking my medication after a few months and my levels are high again I start to get fatigued, headachey, feel like Im overheating. Why would this be happening? Also is there any dangers/side effects for people who have cholesterol as high as mine as the charts in your article seem to stop around 6?
Hi Angela – this article/book may be of interest (https://www.zoeharcombe.com/2013/10/how-statin-drugs-really-lower-cholesterol-and-kill-you-one-cell-at-a-time/) and I highly recommend “Ignore the Awkward” by Dr Uffe Ravnskov. Chapter 3 on familial hypercholesterolemia especially.
If you are 1 of the c. 500 with FH – the bit on FH in that Yoseph post should be of interest. The danger for FH as I see it is that the cells don’t get the contents of the LDL (protein, triglyceride, phospholipids and cholesterol) as they need because the LDL receptor on each cell is not working properly – if at all. The high cholesterol in the blood is a symptom of cells not getting what they need. It is a marker rather than a cause. I hope this explains the danger question you ask – the danger is that your cells are not getting what they need.
Your lifestyle and way of eating seems ideal. The description you give of how you feel off meds is very strange and I can’t think of a logic for it. One of the most noticeable side effects of statins is fatigue and muscle ache, because every cell of the body needs cholesterol and there are consequences to impairing the body’s production of it. Do you have an open minded GP that you could discuss this with? I would expect 99% of docs would put someone with high cholesterol on statins without knowing how they work or what’s really going on with FH. It is so wrong that patients cannot get a considered view on this from doctors. Most GPs still think there’s such a thing as good and bad cholesterol for goodness sake!
Good luck looking in to all this
Very best wishes – Zoe
Is there anywhere on your eye popping site where you suggest what actually IS a healthy diet for ageing people? Personally I note that when I eat light vegetarian food I feel healthier and have less gut inflammation. According to what you have written above this is not recommended by you. Can you clarify?
Thanks
Hi Sally – there is only one way to eat no matter what age you are – real food! The only nutritional debate that we should be having is – should that real food be animal based or plant based? I go through the debate and evidence c. 45 mins in to this video (you may enjoy the whole thing)
There is also a page on this site that I did for farmers – to help them defend the ludicrous attacks on their produce that they get. This may help you decide where the nutrients that you need for optimal health are found.
Modern fibre is far more likely a cause of gut inflammation than the meat we have been eating for 3.5 million years. Only foods of animal origin have essential fats and complete protein and the fat soluble vitamins in the form that the body needs them (retinol, not carotene for example). These are nutritional facts. How you feel is subjective and if you feel better eating this way – it’s your call but do take supplements if you’re avoiding animal foods. You need 39 eggs daily to get 15mcg of vitamin D or you need to sunbathe all year round or you need a small can of sardines many days.
Best wishes – Zoe
Pingback: The Steaming Pile of Shit the Heart Foundation Call Heart Healthy Eating Advice | The Big Fat Truth
Pingback: Everything You’ve Been Told About How to Eat Is Wrong « WORDVIRUS
Hello. I have a grandfather that had a heart attack. Do you know a true way to lower his risk? I read most of your topic and it is simply fascinating! I really hope you can tell me this.. I worry for him and if lowering his cholesterol will kill him then i really am worried.
Hi Jeremy – I’m really sorry to hear about your grandfather. We just had a brilliant presentation by Dr Malcolm Kendrick at our conference and he went through the evidence for different risk factors. The strange thing is that all the ones that the medical profession measures and worry about (salt, cholesterol etc) have no association and there are things that are not measured that have huge association – heart beat regularity being one (perfect regularity is very bad news). Malcolm majored on the impact of stress/the HPA access and more.
The video is in our club for subscribers (http://www.theharcombedietclub.com/forum/content.php?1029-2013-Harcombe-Conference-Dr-Malcolm-Kendrick-Part-1)
I’ve emailed you on the email entered for your blog comment asking for your address and I’ll send you a DVD.
Very best wishes – Zoe
Pingback: Everything You’ve Been Told About How to Eat Is Wrong | Talesfromthelou's Blog
Pingback: Everything You've Been Told About How to Eat Is Wrong
Hi Zoe, I looked at the list of contraindications for Lipitor( Atorvastin)
Two things on the list are being over 70 and having kidney problems.
My uncle is 79 and has kidney trouble and is on Teva Atorvastin. I looked at online info for the Teva product and these things are not listed as contraindications other than a claim that the safety of their product in over 70’s is similar to that in younger patients and that the question of kidney problems should be discussed with the doctor????
Hi Seán – I would definitely raise this with the doctor. I too have seen the contraindication for over 70’s. I have also seen the evidence for high cholesterol and low mortality and low cholesterol and high mortality in all people (hence this blog) but particularly in older people. I thought that even statin lovers acknowledged that you don’t want to be lowering cholesterol in elderly people but some people are either ignorant or conflicted or both – there need to be law suits to stop this
Good luck
Best wishes – Zoe
Pingback: We Don’t Know What to Eat - Informant Daily
Pingback: We Don't Know What to Eat
Zoe, if what you say about cholesterol levels not being affected by the foods we eat is true, then I’m wondering how you would explain what happened to me and two people not related to me after 5 weeks of eating vegan, including low sugar and low sodium:
Person #1, male: lost 39 points of cholesterol
Person #2, male: lost 40 points of cholesterol
Person #3, female: lost 10 points of cholesterol
This is a sincere question and I’d like your opinion, thanks.
Hi Anne
First – please don’t ever think that the cholesterol test is accurate. It has a known error of c. 15% so you can have a cholesterol test one day and it be very different the next day. Two cholesterol tests on the same day will also be very different. This is not a precise science.
If all 3 people are based in the Northern hemisphere, cholesterol falls with sun exposure (vitamin D is made by sunlight synthesizing skin cholesterol). Hence all sensible people who get sun exposure should find their cholesterol levels fall over the summer and rise naturally over the winter.
I don’t say anywhere that cholesterol levels are not affected by the foods that we eat. I say that cholesterol in food makes no difference to cholesterol in the blood – quoting Ancel Keys – and no one has proved otherwise. Since cholesterol is only found in animal foods, a vegan diet has no dietary cholesterol – but this make no difference whatsoever anyway.
What I think has happened is:
1) The article does say “carbohydrates can impact VLDL levels” and, by going low sugar, you have made a very good dietary choice and this will have impacted VLDL levels and hence the overall cholesterol measurement. This bit is good (The fact that you have dropped sugar is good – what has happened to cholesterol is just a sign – not good or bad per se).
2) You have likely eaten more plant sterols (the plant form of cholesterol in effect). These are known to compete in the gut with human cholesterol (hence why things like oats can claim that they lower cholesterol). This is not a good thing. You can find out more on this one in this post (https://www.zoeharcombe.com/2013/01/the-british-heart-foundation-flora-pro-activ-an-unhealthy-relationship/) – the sub heading “how spreads lower cholesterol” is particularly relevant.
So, cholesterol test inaccuracies aside, this is a combination of whatever sunshine the 3 people have had, the good move of lowering sugar and the bad move of having plant cholesterol impact the cholesterol that our body makes for good reason.
Hope this helps
Very best wishes – Zoe
p.s. and don’t forget – low cholesterol equates to higher mortality!
Correlation does not imply causation, please do not change your healthy plant-based diet based on one limited study! There is much research (using data which allows us to draw stronger conclusions) demonstrating the benefits of a whole-foods plant-based diet. I’m not saying we should ignore the study discussed in the article, but to recommend people disregard the relationship between cholesterol and health on the basis of a single correlation-based study is misleading and downright irresponsible.
this is not one study this is the entirety of all studies ever and then another biased study that your ideas are based on being debunked and then another study debunking them again. sterols increase risk of heart disease. They are not the totality of a plant diet, getting rid of sugar will make for less vldl so less circulating. All of these studies I think found that refined sugar was the most detrimental factor.
carbohydrates increase LDL receptors due to insulin signaling t4 conversion to t3 which regulates ldl receptors but having no nutrition with the carbs causes transport issues in the liver, choline is needed for lipoproteins a lack of it can incur fatty liver which will leave you with less cholesterol but not in an ideal situation.
Pingback: Do I Need Meat? Part 1: The Evolution Argument : Cat Food is Good For You
hi Zoe
Even though, even though i’m one of your “radicals” and happy to be, I still believe for all the good science that you show, even down to showing the different metabolic pathways travelled by carbs and fats, nevertheless, you have remain silent on the real issue, which is the impact of “excessive” blood levels of Lipoprotein build up.
Dr Kendrick covers the issue of “excessive” glucose level impact on liver disease – Re: the recent BBC programme.
However, both He and Your good self have remained silent on the issue of the impact of how “excessive” blood lipoproteins levels whether from saturated or other fats also impact the liver also.
As you know Zoe, the problems with Carbs is the “excessive” amounts the body has to deal with. The same with fats. How does the body deal with “Excessive” amounts. does Fat because of its higher Calorific value impact the greater of the two when in “excess”
The issue with fats of all sorts as it is with carbs of all sorts is when both are in “excess” is one a great risk than the other given that “Excessive” levels of Fats produce twice the Calorie value per gram which means 10grams of “excess” fats of all sorts will result in 90 Calories of stores triglycerides, as against 40 calories from 10grams of sugar.
Your thoughts please
Regards
Will
Hi Will – don’t confuse dietary fat with lipoproteins – that’s what the cholesterol theorists want you to do. The two are completely unrelated – as Dr MK says – it is biologically impossible for saturated fat to turn into LDL – a fact that has escaped 99% of GP’s and cardiologists!
There are only two circumstances that I can think of when lipoproteins will be “excessive” i.e. more than there should be:
1) When someone has Familial Hypercholesterolemia. This means that they have a defect on chromosome 19 and their LDL receptors are impaired in their functioning – sometimes to the point of barely being able to take any LDL from the blood stream at all. This will leave far higher levels of LDL in the blood than ‘normal’. I personally don’t see this as the problem per se. I see this as a symptom of the fact that the LDL receptors are not working. Hence the vital components of LDL (cholesterol, protein, phospholipids and triglyceride) don’t get to the cells where they are needed. They remain in the blood. The harm is done in the fact the lipids don’t get to where they are needed – not that them being in the blood is a problem per se.
2) The other circumstance can be where someone has a diet unnaturally high in carbohydrate (as anyone who follows the eatbadly plate will have). VLDL is the lipoprotein made by the liver (not LDL) and we know that this rises with carbohydrate (not fat) intake. Hence we can also unnaturally elevate (in your words – make VLDL excessive) by eating what governments tell us to eat.
Other than this the body makes the cholesterol that it needs and lipoproteins carry that cholesterol (and other lipids) around the body to do their vital work. If you have an operation, injury, illness etc – the body will make more cholesterol because you need more repair. That’s not excessive – that’s terrific body survival mechanisms.
Dietary fat and carbohydrate and their respective calories have nothing to do with any of this (beyond carbs being able to impact VLDL). Dietary fat can be used for basal metabolic needs and/or energy so it has a good chance of being used by the body. Carbs can only be used for energy and we are advised to eat 55%+ of our diet in the form of carbs when we need rarely more than 25% of our diet for energy (and this can be met from dietary fat or body fat – we don’t need to even eat 25% in the form of carbs). While fat is easily used by the body and carbs aren’t – any carbs not used up are converted to body fat (not blood fats – body fat).
Eat fat and hope this helps!
Best wishes – Zoe
Well, there are serious confounding factors in WHO graphs and your inerpretation of them: a.o. level of healthcare standards, availability of healthcare: people from third world have lower cholesterol, but also lower availability of quality healthcare, thus higher probability of CHD mortality. That explains the results and says nothing about real link between cholesterol and CHD mortality (which is clearly established in relevant scientific journals – just google it /and yes, this relationship is positive linear/)
In case you would publish WHO graph which would show relationship between BMI and lifespan, you would very probably obtain similar flat line, or even declining line ! – which does not mean that BMI and longevity has no relationship, or that high BMI is protective factor of longevity, but that confounding factors (=malnutrition, epidemic diseases, many infant deaths, level of hygiene, and unavailability of healthcare in less developed countries) play the role in short lifespan, thus shortening the lifespan of people with low BMI (which hungry people in Africa usually have).
Your other interpretations are similarly flowed from methodological view. I must say I especially “admire” cited rebel doctors who perfectly knows about cholesterol myth (getting rich selling bestsellers about it because people prefer to read about how eggs and red meat is healthy to reading about necessity to eat vegetable…). What is obvious – they do not know anything about scientific methodology. Just consult medical journals and responses to such “experts”. But OK, it is free market of ideas, everybody has right to choose.
Esselstyn, Make yourself heart attack proof achieves rock bottom cholesterol levels through a plant based no fat no oil diet.
http://www.youtube.com/watch?v=AYTf0z_zVs0
Nathan Pritikin cured himself the same way.
Dean Ornish is treating people this way too nowadays. He is paid by Medicare and 40 private health funds because this is cheaper and better than stents and by-passes.
In terms of Hunter and Gatherer diet, the Gatherer is by far the healthiest on all fronts.
Regards, Peter.
Curious you brought up Pritikin – a longevity researcher who died relatively young at age 70. Meanwhile he denied himself many pleasures by his strict diet.
Hi, Zoe
I was searching around the internet looking for statistics that attempt to show correlations between cholesterol levels and actual death rates due to heart attacks and strokes (CVD, in general) and I found your page here. Very nice info!
In November 2011, at 55, I had a “severe coronary event”. It came and went over a 45-minute period and left me wondering what it was. None of the symptoms really pointed to a heart attack, so I went about things as if it was just some curious thing that happened in my body. The next day, just to be sure it wasn’t anything big, I stopped at the doctor’s office and said I had some chest pain the night before. Within an hour they were flying me across town to the Cardiac Intensive Care Unit and the next day performed an angiogram and ultimately inserted a stent in my LAD artery, which they said was 95% blocked.
My cholesterol levels have always been high, as have my parents and grandparents. But there’s no history of heart attacks or heart problems in my family. Indeed, my grandparents all died between 86 and 96 — all with high blood pressure and high cholesterol levels. Imagine that! So it was very puzzling to me WHY this even happened to me.
Of course, from my doctors’ perspective, it was simple: my cholesterol levels.
It turns out I’m very sensitive to most statins as they make me feel like I’ve got the flu, so I prefer not to take them.
Before the heart attack I was on pravastatin as my sister reported it helped her and didn’t make her body ache either. The heart Dr. put me on something else after the heart attack, and it made me miserable. She changed it from one to another, finally going back to the pravastatin. None of which produced the drops they wanted to see — basically because I’m unwilling to spend my life walking around feeling like I’ve got the flu every day! (That feeling like all of my muscles and joints ache, as if I’d been beating with a baseball bat all night long…)
Anyway, last November I started to see a nutritionist because, while I felt my diet was “good”, my blood work was not reflecting what I felt it should. I don’t like taking drugs, so I thought I’d see what a nutritionist could accomplish.
Now, I’m a little overweight (10 lbs or so), but that has never been much of a concern. The nutritionist put me on a diet to ostensibly improve my weight, although it didn’t help. But … my blood work has improved significantly! Over the first 2 months, my blood glucose dropped 7 points, and my lipids improved more than they ever did on the statins. Over the next 2 months, my blood glucose remained flat , and my lipids have improved further — all are within 2 pts (or better) of what they should be “normally”. Except as my GP points out, since I’ve had a heart attack, my targets for those numbers are all really HALF of what is considered “normal”.
(Note that I’ve been getting VAP tests for my lipids since I read about them in a book, giving me a much more detailed look at my lipid stats. The Docs don’t seem impressed.)
What a racket these folks are running!
When I began to see the nutritionist in mid-November, I stopped taking my statins altogether. In January I stopped taking my cardiac meds — because I was given a drug-eluded stent, they told me I had to take them for 12 months, and I stopped after 14 because they refused to cut me off because my cholesterol levels were too high, (mainly because I refuse to take heavy doses of the statins) which is BS as far as I’m concerned.
My cardiologist wasn’t happy when I saw him in February, but he couldn’t argue with the results. So he told me to keep getting my blood tests every 2-3 months and keep doing what I was doing, and he’d see me again in November. (He did his level best to convince me I *NEEDED* to be on SOME kind of statin, which I basically refused.)
Anyway, one thing I’ve discovered that nobody is talking about is L-Arginine supplements. I’ve been taking an L-Arginine complexor since a month before my heart attack, and I was told by one doctor it may have been what kept me from dying. L-Arginine triggers the production of Nitric Oxide in the endothelium, which acts as a vasodilator, an anti-inflammatory, and helps move oxygen from the blood into the tissues. It also dissolves (slowly) plaque build-up, including calcified plaques.
The Nobel Prize in Medicine was awarded to three guys in 1998 for discovering the role that NO plays as a signaling molecule in the endothelium. You’d think that might be a Big Deal in the medical community. But the sad fact is, while NO is turning out to play a very important role in our overall health, it is produced by a NUTRITIONAL SUPPLEMENT. Meaning the drug companies, the FDA, the AMA, and most doctors aren’t going to pay the least bit of attention to it.
(L-Arginine is produced naturally in our body, and we get some from the foods we eat, but not enough. Research has shown that once we hit 30, the amount of NO produced in our bodies drops by 50% for every 10 years we age. So by incorporating L-Arginine supplements in our diet, older folks will begin to see improvements in overall health and well-being simply because the increased NO production allows the body to do what it was designed to do originally, just more effectively.)
When I’ve asked my doctors about L-Arginine and Nitric Oxide regarding my heart condition, they mostly just shrug.
I figured that must be because there isn’t much research on it. WRONG!
If you search PubMed for citations on “cholesterol” you’ll find around 220,000 hits.
If you search for “arginine” and “nitric oxide”, the combined hits are nearly 250,000! Granted, there’s probably a high overlap between them because they’re so closely related, but …
A search on “statins” returns a paltry 25,000 hits.
Obviously, there’s plenty of research being done on L-Arginine and Nitric Oxide around the world and most of it concludes one thing: increased NO production dissolves plaque, leads to improved vascular function, reduces the incidence of both heart disease and its side effects (heart attacks and strokes), and leads to reduced deaths of all causes. It also reverses insulin resistance, improving the body’s ability to metabolize what’s there and reducing the need for insulin injections by diabetics.
What triggers NO production? L-Arginine supplements.
I’ve been taking this stuff since before my heart attack. Over the past 9 months, I’ve also been using a small device that plugs into my computer called a plethysmograph to measure my arterial health. While this device provides the most direct measure of arterial health you can get next to an angiogram, NO DOCTORS IN AMERICA USE THIS INEXPENSIVE EQUIPMENT!
If I ask for another angiogram to PROVE CONCLUSIVELY that the L-Arginine is doing a better job than statins ever can, they say, “it’s not a medically necessary procedure”. If I want to prove this, I’ll have to fork over $5k for an angiogram out of my own pocket.
And don’t even THINK of asking the insurance company to pay for this stuff because it actually WORKS — they don’t even want to KNOW if it works! And they certainly don’t want to pay for something that might improve your overall health and reduce other risks of both disease and death significantly. Uh, remind me what their objectives are again? Oh, yeah … to make money for their shareholders (rather than improving the health of plan participants).
Something is really F’ed up with our medical system. No doubt about it.
Hi David – wow! Thanks SO much for sharing this – what an incredible story.
1) You may find this interesting. It comes from this article (number 1247) only available in abstract currently.
2) You may find the facts about LDL and heart attacks interesting too – The objective of a study called CHEST was as follows:
“To define the clinical profile of young adults with optimal low-density lipoprotein (LDL) cholesterol levels who present with acute myocardial infarctions (MIs); to compare and contrast differences in the clinical profiles of young adults admitted to the hospital with MIs who have LDL cholesterol levels < 100 mg/dL and those with LDL cholesterol values > 160 mg/dL.” i.e. to test LDL levels in people who arrive at hospital having (had) a heart attack.
The conclusion of the study was:
“Young adults experiencing acute MIs typically have acceptable cholesterol levels (i.e.< 130 mg/dL) or optimal values (i.e. < 100 mg/dL)”. (Kwame O. et al, Chest 2001;120;1953-1958) The initial CHEST study was quite small, but the goal was considered to be important to understand. Hence the net was cast more widely to gather far more data on cholesterol levels of people admitted to hospital with heart attacks. Data was subsequently gathered from 231,986 hospital admissions, across 541 hospitals. The lipid levels were documented in 136,905 cases (allowing for VLDL, LDL, HDL etc levels to be known). The average LDL levels were 104.9mg/dl. In UK speak this is 2.6mmol/l. (American Heart Journal 2009;157:111-7.e2) The average LDL level for Americans aged 20 and above entering a hospital because they were having a heart attack was 123mg/dl (2006).
70% of the people admitted to hospital having a heart attack had an LDL level below the average (the “mean” for the statisticians among us). Half of the people arriving at hospital with a heart attack had an LDL level below 100mg/dl (2.5mmol/l in UK language). Hence, people with so called ‘optimal/ideal’ LDL levels were at the same risk of MI (heart attack) as people with higher LDL.
You would think that, with such a magnitude of data and overwhelming evidence, the conclusion would be – one’s LDL appears to have bugger all to do with one’s chance of having a heart attack, Except, perhaps, low cholesterol may not be as favourable as high. The conclusion was, however, that these findings may provide support for even lower LDL goals!
As Dr Malcolm Kendrick said – we can lower LDL to the extreme (zero) and we’d all be dead.
3) Talking of Dr MK – here’s a blog that may depress you, but not surprise you – read the essay at the end – sounds like this is what happened to you.
Well done for looking after your own health – sorry you’ve been let down so badly thus far
Very best wishes – Zoe
Very informative article. I’ve read everything I can on both sides of this discussion about Saturated Fat & Dietry Cholesterol and the potential link to blocked arteries and chd. I’m 100% confused as I see intelligent credible people on both sides of this. I tend to believe this blog vs conventional thinking . My own ldl levels go up or down based on my diet of sat fat and dietary C. But ypu point is whIle that might be true, the level of ldl, low or high, is not a factor for artery blockage and chd. You referenced the CHEST study using 100 as the ldl measure that said 50% of heart attack patients had ldl <100 meaning there is as much chance below or above 100. My cardiologis tells me 70 is the new goal. I take the point /joke about zero ldl but do you have the breakdown from the CHEST study as to what % had heart attacks with ldl < 70. In other words..perhaps < 70 really is good protection whereas over 70 it doesn't matter how much over ?
I wouldn’t be having an angiogram too often one of those is equal to 500 chest X-rays, a lot of radiation!
Stunning, clear, and I wish I’d encountered this merciless exposure of bad science, bad diet, bad pharma practices and medical advice years ago.
Peter.
(Onrus River)
(Hermanus)
(South Africa)
Hi, I am 55 yrs of age, female,and have since I was 34 yrs old been pretty much forced by doctors to take statins as my cholesterol remains mostly around 10.5 – 11. I have taken statins off an on for almost 20 yrs, but with pains in my legs or arms and cramps etc always. I finally refused altogether about 1 yr ago after going through many tests with the cardiologist, who finally told me that despite have a cholesterol level of almost 11, my arteries were totally clear, like a teenagers! Unfortunately there are strokes and heart disease in my family, and I have a heart murmur, so I am a little concerned about my high cholesterol, but will never take statins again!
Thanks Zoe! Yes, I’ve read Uffe’s books and I get his news emails. Also, I’ve read Kendrick and Graveline. All of your works are an inspiration for me. And Gary Taubes really got me started down this path with GC,BC. (that epistle took me two years to read what with all it’s references.)
I think of the difference between HeFH and HoFH as similar to the difference between having one kidney and no kidneys. It seems so bizarre to attempt to extrapolate the bad things that happen to HoFH on to HeFH; of course having no functional receptors would likely be a significant problem!
Recently I joined discussions on the website theFHfoundation.org and attempted a discussion around my situation in order to let other FHers know that HeFH isn’t always a catastrophe (of course the site organizers think FH is worse than the AIDS epidemic). The problem is those website patients self-select for both atherosclerotic disease process and FH, so “obviously”, from their discussions, elevated cholesterol and disease go hand-in-hand. I was impressed how readily my input was ignored; I tried to be respectful of their struggles with disease and at the same time suggest that it was appropriate to actually establish whether plaque was forming before doing anything, and to suggest by my example that elevated C cannot be causitive. It is another lesson in human mental processes to see how readily desperate people “ignore the awkward”. Those that even bothered to address my comments were sure that I should get my levels down before it was too late.
I see a cardiologist annually here in Seattle, and each time he presses me to get on a statin. Each time I ask him to at least hypothesize what benefit he could imagine I’d get, since I already have no plaque. Each time he becomes silent for a few seconds and then we discuss something else. And I’ve down-selected to him because he’s the most open minded cardiologist I can find.
So, anyway, I’m still wondering how to get traction within the medical community that HeFH is often completely harmless.
Oops! Should read “what a great website!!”
Hi Zoe! What’s great website? At age 67 I’ve got HeFH and serum cholesterol of 599 (12 or so in mmols?), yet ZERO calcification by EBCT. From my own investigations, I’m convinced there exist a large fraction of us FHers (20-30%) who never develop any plaque at all (!) even in old age. To me it’s kind of like (hypothetically, of course) discovering a cluster of extra heavy life-long smokers who have completely pink, healthy lungs — it should force a person to rethink what causes lungs to go black (ok, ok, i know there are no such lungs), yet I’ve never found anyone in research who’s interested in figuring out why some FHers get no plaque at all. This seems a grievous mistake — there could be a gold mine of knowledge about plaque formation mechanisms in that understanding. So do you have ideas for stimulating research into looking into any of this?
My personal hypothesis for the excess events for some FH men is that there is some bad cardiac genetic material on the short arm of chromosome 19 in the vicinity of the FH defect sites, and that due to that proximity there is a tendency for them to stay together from generation to generation. It blows me away that geneticists know of at least 1200(?) variants of the FH defect, yet there is almost nothing about which variants tend to associate the most with plaque formation and which, perhaps, not at all.
Hi Robert – thanks so much for your lovely comment. Have you come across Uffe Ravnskov yet? He is the founder of an organsiation called The International Network of Cholesterol Skeptics (www.thincs.org) – his book “Ignore the Awkward” has a chapter on FH with some very interesting stats. I’m going to share your comment with him as he will love that a person with FH thinks as you do!
The Yoseph & Yoseph book “How statin drugs really lower cholesterol and kill you one cell at a time” is also fascinating from an FH perspective. As you know an impact of the chromosome 19 defect is that the LDL receptors don’t work effectively. To simplify the pathway described by the Yosephs – when someone is put on statins, the body tries to respond to the crisis that it detects. As cells realise that their ability to make cholesterol has been impaired, they try to take the cholesterol they need from the blood stream. This lowers blood cholesterol levels and ignorant doctors are happy. They know not what they have done.
There is a second way in which the body tries to save itself – it tries to increase the production of reductase, hoping that this may unblock the mevalonate pathway. It can’t. Hence reductase is both stimulated and inhibited at the same time. Who knows how the body responds to this mechanism being totally confused.
So, LDL receptor activity and reductase activity increase in parallel. The LDL receptors work harder to try to get LDL from the blood stream into the cells. The reductase production increases to try to reboot the mevalonate pathway, so that cells can make cholesterol as they are designed to do. Ironically, the most serious form of FH would receive no benefit from statins anyway. As the extreme form is characterised by LDL receptors working barely at all, even the body going into crisis mode, and trying to take LDL from the blood stream with increased LDL receptor activity, will not work if the LDL receptors are not working sufficiently. Hence the LDL will stay in the blood stream with an extreme sufferer of FH and yet the statin has reduced what little chance the FH sufferer’s body had of making cholesterol within the cell.
As you say – geneticists are missing quite a lot!
Keep up your good health and great thinking
Very best wishes – Zoe
Hi there Zoe
I have just been for an asthma check and had a chat with the practise nurse about diet. She was horrified that we eat butter, not marg. She only has butter at Christmas! I told her I didn’t really believe that cholesterol was a problem in heart disease and that sugar and processed food were more of a problem. She presented a picture of furred arteries, clogged up by choloesterol and how many lives have been saved by statins. I have now got a form to go and have the cholesterol test but I don’t think I’ll bother having read this. I have printed your article out and I am going to take it to my GP practise and ask them to read it and comment. Your comment about The Hippocratic oath is a good one! Are statins doing no harm? I don’t think so!
It would be a really good idea to learn a little bit about statistics before pulling arbitrary numbers out of excel and using them to “prove” your point.
hallo zoe ive poped up here today i hope you dont mind. we got my father in law to look at your other blog last night so heres hoping he thinks about it.
you got me thinking more about my own predicament and the fact i have found certain things to be counter intuitive when confronted with perceived health advice.
i have always had the suspicion i would become diabetic. my maternal grandmother had type 2 as has her son and probably her mother looking at photos. My own mother died 9 years ago when her aorta split open – not an anurism but brittle arteries. she was 69.
i had confirmed gestational diabetes at 32 yrs when i was carrying my third child who was born 1 day late weighing nine and a half pounds. i probably also had it with my second child who was nine pounds at 3 weeks early and with my first who was three weeks and 1 day early and weighed just 4 pounds with a minute placenta that was sent off for research.
at the time i had my first child i was a park ranger and was very active cycling 20 miles every day. throughout my 20s and early 30s i noticed i always put on weight when off work though not because of a change in diet. i ate lots of pasta, potatoes and bread ( i love bread) as well as cakes biccies and chocolate. in 2 weeks i could put on 7 pounds easily. but back to work and id cycle it all off again. i put on two and a half stone following a back injury that prevented me cycling for 6 months. then following a years effort to lose weight i fell pregnant at 9st. i put on 4 stone mostly in the last three months when i stopped cycling.
the next 10 years saw 2 more babies and a weight of 14st 10Ilbs until aged 43 i recognised my symptoms and self diagnosed as a diabetic. the doctor said it was unlikely but took a blood reading which was 9.4 and my HbA1C came back 7.9. My total cholesterol was 4.4 with triglycerides at 1.8. by feb 2009 my TC was 3.9 and trig 1.1. Sep 2010 and they are 4.4 and 0.8 respectively. feb 2012 TC is 4.5 no trig reading. July 2012 TC 4.9 and no trig reading. Jan 2013 TC 5.1 LDL 3.3 HDL 1.4 trig 0.4. ratio TC to HDL is 3.64. But of course this is meaningless as they dont measure cholesterol even remotely accurately.
my spotlight on diabetes targets are TC 5 or below, trig 2.2 or below LDL 3 or below. However there is an unwritten rule for diabetics that should aim for TC 4 and LDL 2 be cause we apparently do not metabolise fats properly any more.
I started to buy those branded plant stanol products last spring but as they contain either too much sugar or i can no longer eat bread or potatoes on which to spread them they were a waste of money. and in any case my cholesterol was still rising. After my diabetic review in july i looked again at LDL lowering and HDL raising food stuffs the obvious one being oats. However i noticed that being a low gi food the metformin that i take twice a day was having little or no effect on it with regard the blood sugar. in fact i have come to realise that because metformin is only active for about an hour it has no effect on low GI, med or high GL foods such as those slow release carbs favoured by health professionals and diabetic organisations which remain in the 8-9 levels in my blood sugar 2 or more hours after eating. These foods actually raise my HbA1C levels to over 7. But if i eat low GL, med or high GI foods such as refined sugars found in chocolate, sweets and biccies the metformin works efficiently lowering my bloods to below 7 within 2 hours and my Hb A1C levels below 7. Therefore eating flour and potatoes raises long term sugar levels which my body converts to fat deposits underneath the skin and eating refined sugary foods lowers long term blood sugars and i lose weight!
I supposedly take metformin morning and evening but in truth i take it whenever i think it will best work and sometimes thats three times and sometimes its once or twice.
now i know so much more about diabetes i realise my mother must have had it undiagnosed for years. some times the medical profession is too clever and looks too much at the minutiae and pays too little attention to the long view.
probably the best i can do for my overall health is get down to 11 and a half stone then ill have a 25BMI and a dog so that i am excersing off my evening meal. i dont want to live forever. there is diabetes, cancer, schizophrenia and senile demetia going back just 2 generations. do i really need to worry about the cholesterol too? when school bangs on about healthy eating to mu cgildren i merely point out that if all they ate was carrots they would soon die! everything is on the menu. Everything in moderation and nothing to excess.
Keep the fight going Zoe it is criminal what both the food industry and pharma companies are doing and with full knowledge just to ‘make a fast buck’. they really dont care that they are killing us all.
rebecca xx
One question Zoe, and I’m sorry if I missed it if it’s been discussed before. Why is it that I have witnessed people lowering their cholesterol through diet change? Doesn’t this indicate that there is some correlation between diet and cholesterol levels?
Hi Tim – good question. There are a number of ways in which diet can impact blood cholesterol levels, but I’ve not found any so far linked to fat.
The most significant relationship is between carbs and triglycerides (VLDL) (Elizabeth J. Parks, “Effect of dietary carbohydrate on triglyceride metabolism in humans”, The Journal of Nutrition, (2001).) The starting substance from which cholesterol is made is called Acetyl-CoA and this is a by product of carbohydrate metabolism and the Krebs cycle. Hence, cut carbs and VLDL falls. LDL is the residue of IDL, which is the residue of VLDL, so carb consumption impacts LDL (low density lipoprotein). People may make dietary changes cutting out biscuits and cakes, thinking that they are cutting fat – they are more importantly cutting out carbs. If they cut pure fat (oils or lard) out of their diet, it would have no impact on blood cholesterol levels.
Another way in which carbs can impact blood cholesterol levels is that certain fibrous foods have plant sterols (plant cholesterol in effect) and this competes in the gut with human cholesterol. Hence oats, for example, have been shown to lower blood cholesterol levels because some of the plant cholesterol ‘wins over’ the human cholesterol and replaces it. I don’t know about you – but I assume that my body is making the cholesterol it needs and plants have the cholesterol that they need and we shouldn’t mess around replacing one with another! (Here‘s a great Uffe article on the dangers of this).
Another way in which I can think of diet impacting blood cholesterol levels is overall health. Cholesterol is our main repair tool, so the body makes more if we have more damage to repair. A high sugar diet would likely cause internal damage requiring more cholesterol to be made to repair – another example of carbs impacting cholesterol, but not fat.
Hope this helps!
Best wishes – Zoe
Zoe
The context I was referring to was your article as a whole. I’m not accusing you of misquoting or misrepresenting Taubes. I’m sorry if I implied that. Obviously the Diet Delusion is not Holy Writ and you’re not obliged to agree with every word of it.
I’m simply pointing out to you and to readers of this blog that an extremely well-known and oft-quoted person in this debate, who is greatly admired by people who take your view, does, in fact, apparently believe that saturated fats raise cholesterol. Having said that, references to it in his book, although unambiguous, occur almost as throw-away remarks. This is odd for such an important issue and it would have been better if he had outlined his views on this in more detail.
I think it’s a bit naive to suggest that non-scientists like me can “decide for ourselves” by making our own assessments of the scientific evidence. We don’t have the knowledge to do that. We have to learn what we can and then make judgements about the comptence, reliability and integrity of the experts’s and we have to decide whther what they are saying seems reasonable.
In the case of Dr McKendrick, it’s not a question of judging him on the basis of any old review. It’s about the specific review I read. This was written by somebody who a) takes Dr McKendrick’s view on the diet-heart hypothesis so is not biased against him, b) is clearly extremely knowledgeable, c) is very fair-minded, writes in a sober style and is clearly not leading some kind of crusade, and d) whose criticisms of Dr McKendrick’s work are specific and detailed rather than general and vague.
So it’s not unreasonable for me to conclude from that that Dr McKendrick’s book might not be the best place for me to start. Which is not to say that I will never read it.
Regards
Edward
Hi Edward – I’m baffled! I refer to Taubes in the context of conflict of interest with cholesterol targets.
This is the passage: “Taubes has a deeply troubling passage in The Diet Delusion where he looked at the committee who approved a lowering of the target cholesterol levels for the USA population. From memory (it’s a big book to find a reference!), a number of people were on the committee and all but one were funded by pharma companies and one didn’t want the target cholesterol level lowered. I wonder which one! (Anyone reading this – if you can find the page number I’d be so grateful – my copy has so many scribbles on I can barely read it).”
Period. No mention of sat fat. No suggestion either way what Taubes’ views may be on sat fat – just respect for his uncovering of a conflict of interest.
Well done trying to come to your own conclusions about health issues but a couple of tips – 1) don’t judge someone as brilliant as Dr Kendrick on the basis of one review on one site – read the original and decide for yourself and 2) don’t make inferences in what you do read that aren’t there.
Best wishes – Zoe
p.s. I never did find this passage again in Taubes book. It can be seen here at c. 43 mins in (http://www.youtube.com/watch?v=3vr-c8GeT34) and there are full details in the Yoseph & Yoseph book “How statins really lower cholesterol and kill you one cell at a time”
I have read Garry Taubes “The Diet Delusion” and it is one of the most fascinating books I have read in my life and is indeed shocking in many places. However, I’m surprised you quote Taubes in the context of denying the link between saturated fat and cholesterol as Taubes clearly states that there is such a link (on pages 156, 175 and, most emphatically, page 164). By the way, I’m not quoting these references from memory – I went to the book and looked them up with the help of the index.
Incidentally, Taubes also uses the shorthand “LDL cholesterol” to mean the cholesterol contained in low-density lipoproteins, even though his book clearly points out the importance of distinguishing between cholesterol and lipoproteins.
I definitely want to learn more about this area. I don’t think I’ll start with the McKendrick book, though, because of the pretty negative review by Chris Masterjohn on the website “Cholesterol and Health”, which is written by someone who basically takes your position on the issue.
As a non-scientist, I cannot evaluate most scientific evidence so I have to make judgements about which scientists are most reliable based on how they write and how they appear to approach the evidence. To be frank, comparing Masterjohn’s measured, sceptical review of McKendrick’s book with your unrestrained enthusiasm makes me a little bit wary of your website.
Regards
Edward Hubbard
I searched for Chris Masterjohn’s review of Malcolm Kendrick’s book. The website, “Cholesterol and Health”, no longer exists, but the review can be read via this link: https://web.archive.org/web/20180104112618/https://www.cholesterol-and-health.com/Malcolm-Kendrick-Great-Cholesterol-Con.html
Having read all Zoe’s articles will be coming off
statins TODAY. Hope to get back to clear thinking soon!
Many thanks for all the info. B.C
I have read your article and it makes a lot of sense, but if it is not Cholestoral that blocks arteries, what does cause blocked arteries? I had a tripple Bypass when I was 44 due to my arteries being blocked.
Regards,
Alan Keen
Hi Alan
I’m very sorry to hear you had all this to deal with and so young.
There are many things that can damage the endothelial wall – the lining of the arteries… chief suspects are smoking, stress, sugar, processed food, chemicals, pollution – modern aspects of modern living in other words.
When damage occurs, a scab forms over the area, just as it does if we cut our finger. However, we cannot allow a scab to break off in the blood vessels – or a blockage could occur – so the incredible body forms a lining over the scab and tries to repair the damage under this cover and so smooth the bump so that the width of the artery returns to normal. If the modern lifestyle continues, damage can form on top of damage – a bump on top of a bump – and the artery can narrow to critical point.
The ultimate irony? The repair kit for the damage is contained in a ‘taxi’ called LDL – a Low Density Lipoprotein. LDL carries protein, triglyceride, phospholipids and cholesterol – all the tools needed to repair the damage. When surgeons opened you up they would have found LDL at the scene of the crime – no doubt confirming their view that LDL had caused the problem. LDL was the solution not the problem. I liken this to police arriving at the scene of the crime – they don’t get accused of committing the crime!
Good luck with making plenty of cholesterol to continue repairing any damage – although I’d bet they’ve put you on statins?!
Best wishes – Zoe
Just read this article via a link on Dr John Briffa’s site. Your article is superb and I must re-read it. I read Ravnskov’s original book and, later, Kendrick’s tome. Great books. I had a small stroke in February (fine now) and the hospital tried to put me on statins. It’s amazing high they struggle with someone who says “no”. My GP tried months ago and he doesn’t bother now.
Anyway, keep up the good work.
Robin
Hey Zoe…. I just went to my doctor for my yearly checkup. Had not been in 3 years because I had quit taking my cholesterol medicine and did not want to hear about it. However, the results came back with my Cholesteral at 354 and my LDL at 259. I will tell you that she was freaking out about this, that mine was the highest number that she had ever seen….. I have read all your articles and think that I am ok. I had an EKG that came back ok. They did not tell me any different. I am 60 years old now so I don’t know if that matters or not. I do exerise 3 X a week.
Keep up the good work.
Sara
Amazing article, but also so scary that ‘respected’ scientists skew the evidence to support their theories. Climate scientists caught out doing the same a few years ago. No wonder the public don’t trust science. Keep on doing what you do. Thank you
Thank you so much Zoe.
Many thanks Zoe – I’ve just bought the Yosef and Yosef book and will buy the one by Uffe as well as it’s the link between FH and cholesterol I need to sort out before my next healthy heart check up with the practice nurse(??!!). If it wasn’t FH then there’s no way I would be taking statins but after being guilt tripped by my GP I’ve been going round in circles trying to decide what to do. I DO know that my mother had a necessary bypass op but did not fit the usual criteria for someone with heart problems – not overweight, good diet, exercised etc. and was put on to statins. We 3 daughters were advised to have a cholesterol test and mine was the only raised level (over 8 mmol). My mother has since been given ever increasing doses of statins to keep her levels within ‘normal’ I don’t want to go down that route but in fact my GP practice now only tests once after starting statins and provided the level has dropped then you stay on statins forever, without any further testing – what sort of medical advice is that?? The time I did stop taking the statins and insisted on another cholesterol test my level went up to over 11 mmol, hence my worries. I’m also trying to research the part that sustained high stress levels have to play in all this. I will read the books you advise, many thanks for your help.
Hi Elsie – I don’t envy you up against the system! Stress plays a significant part in both heart disease per se (The Great Cholesterol Con, Dr Malcolm Kendrick) and in cholesterol readings. Your cholesterol reading will never be the same in two readings. How stressed you are on the day will affect it, as well as stress generally. Running late for the appointment will affect it! Sunshine will affect it, injury (the body makes more to repair you) and more and more.
You may enjoy this blog from Dr Malcolm Kendrick on bypass surgery: http://drmalcolmkendrick.org/2012/04/13/the-joy-of-coronary-arteries-the-body-aint-that-simple/
And here’s an extract from my book “The Obesity Epidemic: What caused it? How can we stop it?” about the actual blood cholesterol test:
“The standard blood cholesterol test does not measure LDL – it estimates it.
“The fasting blood cholesterol test is the traditional way to measure the level of LDL, but it doesn’t measure LDL directly. We can only measure total cholesterol and HDL with the standard blood test and Triglycerides (VLDL) and LDL are together assumed to account for the difference. The estimation is refined further using the Friedewald equation (named after William Friedewald, who developed it). This uses the fact that VLDL is 22% cholesterol to establish the equation:
“Total cholesterol = LDL + HDL + Triglycerides/5 which leads to:
LDL = Total cholesterol – HDL – Triglycerides/5. (Ref 1)
“You can also now see the problem with trying to assert any meaningful relationship between HDL and total cholesterol. Total cholesterol/HDL = LDL/HDL + 1 + Triglycerides/5HDL and we have one equation, with four variables, only two of which can be measured. We need at least one more equation or known variable, to avoid circular references.
“As the November 2004 Harvard medical school publications note, “You have to fast for about 12 hours before the test because triglyceride levels can shoot up 20%-30% after a meal, which would throw off the equation. Alcohol also causes a triglyceride surge, so you shouldn’t drink alcohol for 24 hours before a fasting cholesterol test.” They also caution “At a triglyceride level of about 250 or higher, the Friedewald equation becomes less reliable because dividing triglycerides by a factor of 5 provides a less accurate estimate of VLDL.”
“These complications and inaccuracies aside, the fact that LDL is estimated means that:
– All other things being equal, LDL will rise if a) total cholesterol rises and/or b) if HDL falls and/or if c) VLDL falls.
– All other things being equal, LDL will fall if a) total cholesterol falls and/or b) if HDL rises and/or if c) VLDL rises.
No wonder an inverse association is observed between LDL and HDL – it is by definition. More surprising is that a fall in VLDL (triglycerides), which would be welcomed by doctors, would be accompanied by an automatic increase in LDL, all other things being equal, which would not be welcomed by doctors. There was me thinking this was scientific.
Ref 1: EH Mangiapane, AM Salter, Diet, Lipoproteins and Coronary Heart Disease: A Biochemical Perspective, Nottingham University Press, (1999).
Zoe – do you have a reply for Lynn (above) re the Familial version of raised cholesterol levels?. You said in your report that Uffe Ravnskov has said that high cholesterol is not a risk factor in FH – have you read the referenced papers yet? I’m taking statins with no obvious ill effects but want to stop taking them. I’m worried that there may be a link between FH and CVD but would love to hear that there isn’t.
Hi Elsie – it’s a blog in itself probably! Too many blogs to do, too little time. I highly recommend getting hold of Uffe’s books – especially the latest one “Ignore the Awkward”. There’s a chapter about FH and he’s the expert on it.
The book that I’ve just finished reading would also help – “How statins drugs really lower cholesterol and kill you one cell at a time.” (Yoseph & Yoseph) One of the most shocking books you’ll ever read on conflict of interest and the scandal that is statin drugs. In short – statins block the mevalonate pathway in the body, which is just about as serious as anything we could do to another human. This stops cell rejuvenation, production of isoprenoids – including the one responsible for DNA replication and cell replication and also CoQ10 – vital for energy. The body responds to this life threatening situation by increasing production of reductase. (Statins are called reductase inhibitors – and they are – but they are also reductase stimulators, as the body will try to make more reductase to reboot the mevalonate pathway. This doesn’t work, by the way. Nothing can reboot the mevalonate pathway – this is why we will be killed one cell at a time.) At the same time as reductase tries to rescue the body, the LDL receptors also try to take more LDL from the blood stream into cells to protect those cells. This is because the cell recognises that it can no longer make its own cholesterol properly, as this has been impaired by statins (statins don’t stop the body making cholesterol entirely or they would kill us instantly). Hence statins increase LDL receptor activity, as the body tries to get the LDL needed by the cell from the blood stream. This is how LDL in the bloodstream is lowered – it has been taken by the cells in response to the attack the body has experienced and to replace the cholesterol that the cell would have happily made if left alone.
FH is characterised by a gene defect on chromosome 19. In some types of FH, the LDL receptors barely work at all and statins won’t help with this type at all because, even with the LDL receptors being stimulated to take more LDL from the blood stream, the receptors are just not working well enough to do this. (The early supporters of statins know this by the way – they know exactly how statins do their worst and they know that they won’t help the most serious type of FH. Statins, ironically, were only originally approved for FH, but the money is in being able to prescribe them for anyone with a pulse.) In other types of FH, the LDL receptors work to an extent and the stimulation of the LDL receptors can help to get more LDL into the cells. This might be a good thing but for the fact that the statin has stopped the cell producing its own cholesterol and but for the fact that the statin has blocked the mevalonate pathway and thus shut off cell rejuvenation and the cycle of life itself.
I know that I will never, ever, ever take a statin and I wonder if any doctor would prescribe them ever again if they read everything that we know about these drugs.
Ignorance is not bliss when it comes to the mevalonate pathway!
Best wishes – Zoe
p.s. since writing the cholesterol and heart disease blog, I thought of another bit of logic – high cholesterol is not a problem in itself – the problem with FH is that the LDL (the lipoprotein carrying cholesterol and protein and phospholipids and triglyceride) cannot get into the cell effectively, as the LDL receptor is not working properly (or at all). This means that the damage done to the body is because the vital LDL – our body’s repair kit – doesn’t get to where it should. This can include not getting to the heart and other vital organs – as every cell needs cholesterol and the other substances in a lipoprotein. Hence the heart can be damaged by not getting the repair kit. The repair kit being in the blood stream is not a problem per se – it’s a symptom of the thing that didn’t happen being a problem!
Things can be seen very differently when you don’t start from the assumption that cholesterol is evil!
Zoe – how absolutely fascinating, and also incredible – how can anyone still subscribe to the idea of lowering cholesterol even further? My own level is 4, tested just after my husband had his heart attack, and the nurse was ecstatic, saying how wonderful that was, and to keep up the good work. The truth is, I do nothing in respect of my cholesterol level – I eat butter, eggs, cheese, whole milk (I object to it being called “full fat”), red meat, poultry – you name it, it is on the opposing side from the “healthy” eating edict!! I didn’t let on to the nurse, because I knew she would be horrified, simply because what I eat is not considered by the establishment to be conducive to a healthy heart. I, too, have long believed the “saturated fat is the devil” brigade to be totally deluded. An incredibly clever, prolonged and guilt-inducing campaign has been waged against us mere citizens in respect of what and how we eat, and none of it is because anyone is remotely concerned with our health…..
Hello! My husband had a mild heart attack on New Year’s Eve, and left hospital fully equipped with Simvastatin, plus other probably strong drugs. Up until three weeks ago, when he refused to take any more statins, he was in great pain in his knees in particular (those joints are arthritic in any case, so it was almost unbearable for him). Literally within 24 hours, the pain had eased enormously. I had shown him a document written by a well-known lady heart specialist, which states much the same as you, Zoe, in respect of statins and cholesterol. What totally flummoxes me is that his cholesterol level was below four BEFORE he had his heart attack, so I am at a loss as to how anyone, let alone doctors, can categorically state that any sort of cholesterol has anything at all to do with heart disease. Our GP has now given him Provastatin – I’m rather kicking myself, because I felt that he shouldn’t just stop some of his medication without consulting our GP (who’s brilliant, but clearly still on the statin bandwagon). At the last check, my hubby’s cholesterol was 2.1 (that was six weeks after his heart attack). The price of that, of course, was unbearably painful joints, and chronic tiredness. I wholeheartedly denounce the suggestion that people of any age should be routinely given statins. The document I read, and gave to my husband, suggests that we are sitting on a potential time-bomb with regard to these drugs. And yes, of course the drugs companies want the current panic to continue – they’re making nice fat profits out of it. What also irritates me is the mis-information about cholesterol generally. As far as I can tell, we’d actually die without it! And how on earth can it be a good thing to prevent a natural process within the body, which results in having to introduce other substances (co-enzyme Q10 springs to mind)artificially? I bet the producers of Q10 are also rubbing their paws lasciviously!! Perhaps people should be advised to read the history of the occurrence of heart disease in this country (widely available in libraries and on the internet), and note that it pretty much coincides with the introduction of many processed foods, and nonsensical warnings about fats. You may have noted that I’m rather outraged! We should ALL be outraged by this.
Hi Catherine – what a passionate and heartfelt note – I am appalled to hear this and you are right – we should all be outraged by it. The latest book I’ve just finished “How statin drugs really lower cholesterol; and kill your body one cell at a time” is the most shocking book on this topic that I have yet read. By Yoseph & Yoseph – I just wish some doctors would read it and get off the statin bandwagon!
Good luck to you and hubby
Very best wishes – Zoe
p.s. here’s an extract from an article I wrote for our on line club (www.theharcombedietclub.com) after seeing Dr Malcolm Kendrick present at the 2011 Weston Price Conference in London:
“The finale in this fat/heart/cholesterol section was a study on cholesterol, which I had not previously come across. This was a study called “CHEST” (you will notice that every study has to have a name and rarely are the names a logical abbreviation of something e.g. MONICA is the name for the “Monitoring Trends In Cardiovascular Disease” study).
The objective of CHEST (http://chestjournal.chestpubs.org/content/120/6/1953.full.pdf) was as follows:
“To define the clinical profile of young adults with optimal low-density lipoprotein (LDL) cholesterol levels who present with acute myocardial infarctions (MIs); to compare and contrast differences in the clinical profiles of young adults admitted to the hospital with MIs who have LDL cholesterol levels 160 mg/dL.”
The conclusion of the study was:
“Young adults experiencing acute MIs typically have acceptable cholesterol levels (i.e.< 130 mg/dL) or optimal values (i.e. < 100 mg/dL)”. (Kwame O. et al, Chest 2001;120;1953-1958)
The initial CHEST study was quite small, but the goal was considered to be important to understand. Hence the net was cast more widely to gather far more data on cholesterol levels of people admitted to hospital with heart attacks. Data was subsequently gathered from 231,986 hospital admissions, across 541 hospitals. The lipid levels were documented in 136,905 cases (allowing for VLDL, LDL, HDL etc levels to be known). The average LDL levels were 104.9mg/dl. In UK speak this is 2.6mmol/l. (American Heart Journal 2009;157:111-7.e2)
There was a great slide presented by Dr MK (which I can't work out how to replicate here!) The graph shows the average LDL levels for Americans aged 20 and above, in 2006, entering a hospital because they were having a heart attack. This graph shows that the average LDL level for these Americans was 123mg/dl ( http://health.usnews.com/usnews/health/articles/061219/19parkinsons.htm ).
70% of the people admitted to hospital having a heart attack had an LDL level below the average (the “mean” for the statisticians among us). Half of the people arriving at hospital with a heart attack (MI is the technical term) had an LDL level below 100mg/dl (2.5mmol/l in UK language). Hence, people with so called ‘optimal/ideal’ LDL levels were at the same risk of MI (heart attack) as people with higher LDL.
You would think that, with such a magnitude of data and overwhelming evidence, the conclusion would be – one’s LDL appears to have bugger all to do with one’s chance of having a heart attack, Except, perhaps, low cholesterol may not be as favourable as high. The conclusion was, however, that these findings may provide support for even lower LDL goals!
As DR MK said – we can lower LDL to the extreme (zero) and we’d all be dead.
I sent an email (in the wrong place) about my husband’s problems with the medical people. They are, on the whole, absolutely entrenched in this theory that cholesterol causes heart disease and unless you take statins you are the villain of the piece. It makes you want to never visit a doctor ever again. I never go to surgery unless forced to, because I do not wish to be caught in the ‘statins’ trap. My 80 year old lady friend was put on them by her doctor and apart from leg pain, cramps and a bad back, she was driven down to a level of 2. l/2 so the doctor suggested she took a months break then started again. Can you believe it?
It’s an nightmare actually.
Hi Sue – that has got to be medical malpractice. Download the patient leaflet for Lipitor (the one that has earned Pfizer c. $125 BILLION since launch).
The leaflet actually states “Take special care with Lipitor. The following are reasons why Lipitor may not be suitable for you…” Final bullet says “If you are older than 70 years”. This caution is because we know that the brain hosts 25% of the body’s cholesterol and we know that older people are more prone to Alzheimers, memory loss, loss of cognitive ability. It’s because we know that every cell of the body needs cholesterol for health and older people are more prone to immobility and muscle aches and pains and it’s because we know that study after study (I reference them in my obesity book) note the evidence for low cholesterol and high mortality and high cholesterol and low mortality – which is what this blog post was about. But hey, don’t let your friend’s life get in the way of statin profitabilty? Absolutely criminal
Stay wise, informed and away from surgeries!
Very best wishes – Zoe
My high cholesterol is hereditary, so I believe, my Mother suffered from multi infarct dementia due to arteriosclerosis ….due to high cholesterol ( didn’t eat lots of saturated fat but did eat meat and dairy). So what should I do now? I have stopped statins as I had bad side effects even though I took co enzyme Q10. Am I going to suffer the same fate as my Mother? According to this article how does this affect me?
Wow. Well done.
This is a brilliant article, I have been banging on about this issue for years now, to always be looked at like I was a lunatic who knew nothing and had just landed from Planet Zob.
Well done to you